Explore effective stenosis treatment without surgery. Our 2026 guide covers non-surgical options: spinal decompression, PT, & more for lasting relief.
You may be there right now. You can stand long enough to make coffee, but a walk through the store turns into a search for the nearest bench. Your back tightens, your legs start to burn or feel heavy, and leaning forward over a cart gives you more relief than standing upright. Over time, life gets smaller. You choose shorter outings, skip the things you enjoy, and wonder if surgery is the only real answer.
For many people, it isn't.
Spinal stenosis means the space around the nerves has narrowed. This condition resembles a tunnel that has gradually tightened around structures that need room to move. That narrowing can irritate nerves, limit walking tolerance, and create pain, numbness, weakness, or cramping. The good news is that stenosis treatment without surgery can be structured, practical, and evidence-based rather than a random list of things to try.
Good care also depends on feeling heard, informed, and guided through decisions. That's one reason thoughtful systems for communication matter, and Recepta.ai's patient experience insights are useful reading for anyone who wants to understand what makes a treatment journey feel clear instead of confusing.
Individuals with stenosis don't come in asking for a philosophy lesson. They want to know why walking hurts, why sitting helps, and whether they can get back to normal life without an operation. That's a fair question, because stenosis often behaves in a very specific pattern. Symptoms build with standing and walking, then ease when the spine flexes forward or the body rests.
The experience can be discouraging because the pain doesn't always stay in one place. Some people feel it mainly in the low back. Others notice tingling, heaviness, or aching down the legs. Some feel strong when they wake up and limited by midday. This inconsistency makes many patients think something mysterious is happening when the problem is often mechanical.
A useful way to think about stenosis is this: your symptoms are giving clues about what positions reduce pressure and which ones increase it. If leaning on a counter, walker, or shopping cart helps, that matters. If standing still is harder than sitting, that matters too. Those details help guide treatment.
Practical rule: If a treatment plan for stenosis doesn't account for posture, walking tolerance, and movement patterns, it's probably missing the core problem.
The most effective non-surgical approach usually isn't a single therapy. It's a tiered pathway. Foundational care improves mechanics, mobility, and tolerance. Advanced care is added when symptoms are more stubborn or when the underlying disc and nerve mechanics need more direct unloading. That's the difference between trying things and following a plan.
Spinal stenosis happens when the spaces in or around the spine narrow enough to crowd the nerves. The “kinked hose” analogy helps. If a garden hose bends sharply, water flow is restricted. In stenosis, the nerves are the structure being crowded, and the result can be pain, numbness, tingling, weakness, or reduced endurance.
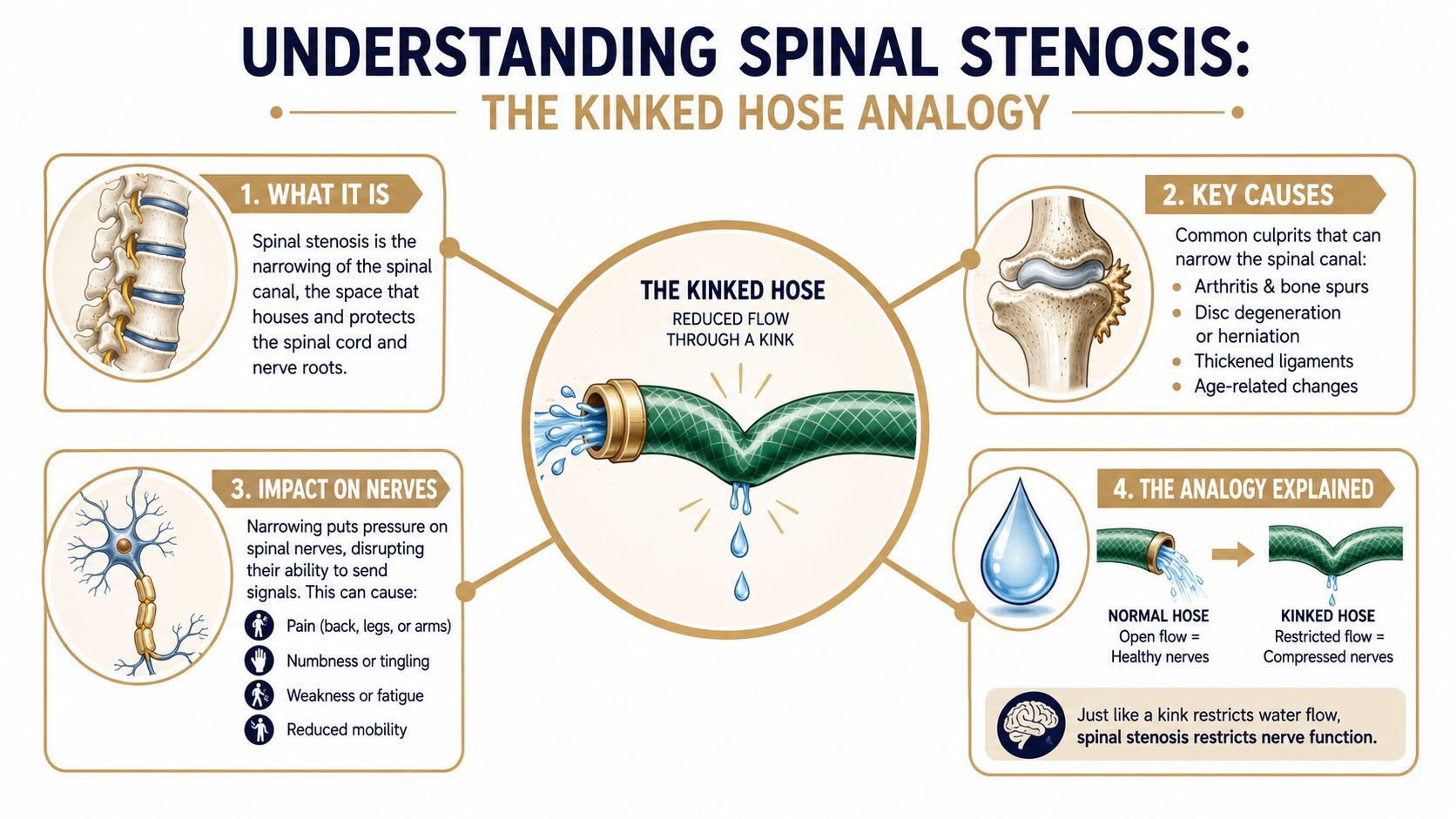
Several structures can contribute to that narrowing. Discs can bulge. Joints can enlarge with wear. Ligaments can thicken. Bone spurs can occupy space that nerves used to move through more freely. None of that means the body is “broken,” but it does mean the available room has changed.
Symptoms make more sense when you connect them to the mechanics:
Lumbar stenosis affects the low back and commonly causes buttock pain, leg pain, cramping, heaviness, or walking intolerance. Cervical stenosis affects the neck and may contribute to neck pain, arm symptoms, hand clumsiness, or balance changes. The location matters because treatment planning depends on which nerves are being crowded and how that crowding shows up in daily life.
There's also an important clinical distinction within lumbar stenosis. In lumbar spinal stenosis patients without instability, non-surgical care can produce meaningful improvement, while certain subgroups, including those with spondylolisthesis, tend to do less well with conservative care. Patients with isolated back pain or single-level stenosis without instability often do satisfactorily with non-surgical management, according to this review of lumbar spinal stenosis subgroups and conservative outcomes.
When patients understand the mechanics, treatment stops feeling random. They can see why some positions flare symptoms and others calm them down.
The first tier of stenosis treatment without surgery should do two things at once. It should reduce irritation now, and it should teach your body how to move with less nerve crowding going forward. That's why the basics matter so much.

Foundational care often begins with activity modification. That doesn't mean bed rest. It means changing how you move so your nerves aren't repeatedly compressed.
A practical plan may include:
Walking while slightly flexed forward is one example of useful modification. Many people discover this accidentally when leaning on a cart helps more than standing upright. That's not a strange habit. It's a clue.
Manual care can help when joints are restricted, soft tissues are guarding, and the body has settled into painful compensation patterns, allowing treatments like Chiropractic Adjustment, realignment, massage therapy, mobility therapy, and guided rehabilitation exercise to work together rather than compete.
A strong trial on multimodal non-surgical care found that a program combining manual therapy, including spinal mobilization, manipulation, and massage, with individualized supervised and home exercise produced significantly better short-term improvement than medical care or group exercise alone. The manual therapy group reached a 20% responder rate at 2 months, compared with 7.6% for medical care in this study on manual therapy and individualized exercise for lumbar stenosis.
That finding matches what many clinicians see. The body usually responds best when passive care and active care are paired.
For patients who need structured progression, rehabilitation exercise programs can help bridge the gap between symptom relief and durable function.
Foundational care isn't “basic” because it's weak. It's foundational because everything that follows works better when movement quality improves first.
Other supportive options may also have a place, depending on the case. Muscle stimulation can reduce guarding. Acupuncture may help with pain modulation. Nutrition counseling can support body composition and recovery habits. These are supports, not substitutes for a solid mechanical plan.
Some patients improve well with exercise, manual care, adjustment, and lifestyle changes. Others hit a ceiling. They feel looser, but they still can't walk far. Their symptoms keep returning when they load the spine. That's often when advanced interventions become more relevant.
Non-surgical spinal decompression is meant to address the mechanical side of pressure more directly than exercise alone can. In practical terms, the goal is to unload the spinal segments in a controlled way. With disc-related narrowing, that may reduce stress on irritated structures and create better conditions for movement and healing.
The DRX9000 is one example of technology used for this purpose. It applies computer-controlled decompression to targeted lumbar segments. Patients often ask whether this is just “traction.” It isn't the same as generic pulling. The treatment is designed to apply specific loading patterns rather than simple force.
Evidence for decompression is stronger in some spinal conditions than others, and that trade-off matters. In a case series involving lumbar intervertebral disc lesions, non-surgical spinal decompression with the DRX9000 achieved an 80% reduction in pain after 20 treatment sessions, disability improved by 50%, and patients reported a 75% overall improvement in symptoms and daily activities, as reported in this DRX9000 clinical case series.
That doesn't mean every stenosis patient is a decompression candidate. It does mean decompression deserves serious consideration when disc pressure, nerve irritation, and walking intolerance are part of the pattern.
For readers looking into this option in more detail, non-surgical spinal decompression care explains how this type of treatment is used clinically.
Advanced care doesn't stop with decompression. Some patients need inflammation management, tissue recovery support, or help calming down stubborn pain pathways so they can tolerate movement again.
That's where modalities can be useful, especially when they're given a clear role:
One clinic option that fits this model is Aspen Falls Wellness, where services such as DRX9000 decompression, MLS Laser Therapy, SoftWave Therapy, chiropractic care, massage therapy, personal exercise plans, mobility therapy, and nutrition counseling can be combined within one care pathway when clinically appropriate.
Advanced tools work best when they solve a specific problem. They do less when they're added just because they're available.
This is the main distinction patients often miss. Foundational care teaches the body to move better. Advanced care helps when the body still needs more direct mechanical unloading or stronger support for tissue recovery. The best plans know when to use each.
A good treatment plan doesn't stack services just to make the schedule look full. It sequences them. The right therapy at the wrong time can be less effective than a simpler choice used well.
A typical patient journey starts with a careful exam and, when needed, imaging referral. The goal is to decide what's driving the symptoms. Is it mainly disc-related compression, stiffness, neurogenic claudication, muscular guarding, inflammation, or a combination?
From there, care is layered:
Nutrition can matter more than many patients expect. Recent multimodal rehabilitation data suggest that targeted flexion-based physical therapy, weight loss, and anti-inflammatory nutrition can reduce lumbar lordosis and slow functional decline in up to 35% of moderate-severity cases, according to this Mayo Clinic discussion of non-surgical lumbar stenosis care.
That's one reason integrated care works better than isolated care. Pain relief without movement training doesn't hold. Exercise without symptom control is hard to sustain. Nutrition support without a mechanical strategy won't fully address nerve crowding.
Patients who want to understand how clinicians structure these layered decisions may find it helpful to explore treatment plan examples and see how different therapies are combined around diagnosis, goals, and re-evaluation. Some patients also benefit from approaches used in acupuncture for chronic pain care plans, especially when pain sensitivity and muscle tension are major barriers.
| Therapy | Primary Goal | How It Works | Best For |
|---|---|---|---|
| Chiropractic adjustment and realignment | Improve joint mechanics | Restores motion in restricted spinal segments | Stiffness, guarded movement, mechanical pain |
| Massage therapy | Reduce soft-tissue tension | Calms muscle guarding and improves tissue mobility | Protective spasm, soreness, compensation patterns |
| Mobility therapy | Increase usable range of motion | Improves movement in the spine, hips, and related joints | Patients who feel locked up or limited in transitions |
| Personal exercise plans and rehabilitation exercise | Build lasting function | Reinforces flexion-friendly movement, strength, and endurance | Long-term symptom control and relapse prevention |
| Spinal decompression | Reduce disc and nerve loading | Applies controlled unloading to affected segments | Disc-related symptoms, walking intolerance, leg pain patterns |
| MLS Laser Therapy | Support inflammation control | Delivers light energy to irritated tissues | Inflamed, reactive tissues that slow progress |
| SoftWave Therapy | Support tissue healing response | Stimulates repair-oriented biological activity | Stubborn soft-tissue irritation or delayed recovery |
| Acupuncture | Modulate pain response | Influences pain signaling and muscle tone | Persistent pain with a strong sensitivity component |
| Nutrition counseling | Support recovery capacity | Addresses weight, inflammation, and daily habits | Patients needing broader long-term support |
Stenosis is usually managed, not erased. That isn't bad news. It's just a more useful way to define success. The goal is less pain, better walking tolerance, improved function, and fewer flare-ups.
Patients often want a hard deadline, but stenosis doesn't follow a perfect calendar. Some people notice early changes in standing tolerance or morning pain. Others improve more gradually as the spine becomes less reactive and movement confidence returns. Consistency matters more than speed.
Long-term research helps frame the trade-off. Surgical decompression tends to provide stronger early improvement, but outcomes between surgical and non-surgical groups often move closer over time. Surgery still remains associated with better long-term leg pain relief and walking capacity beyond five years in this long-term review of surgical and non-surgical lumbar stenosis outcomes.
That's the balanced message. Non-surgical care is often a very reasonable first path. Surgery still has a place.
Some symptoms should never be “worked through” with routine conservative care. Get urgent medical evaluation if you develop:
If strength is dropping fast or bladder and bowel function changes, this is not optional. Seek immediate medical care.
Surgery also moves higher on the list when pain and disability remain severe after a thorough course of non-surgical treatment, or when neurological deficits continue to progress despite appropriate care.
Symptoms can return because stenosis is tied to ongoing spinal mechanics and age-related change. That doesn't mean treatment failed. It usually means your spine needs ongoing management, just like other chronic musculoskeletal conditions. The goal is to reduce severity, improve function, and make flare-ups shorter and easier to control.
Most patients describe decompression as gentle rather than painful when they're properly screened and positioned. It should feel controlled. If a treatment increases nerve symptoms sharply, the settings or the plan may need to change. Safety depends on good diagnosis and proper patient selection.
Diet won't replace mechanical care, but it can influence inflammation, body weight, and recovery capacity. For some patients, that changes how well they tolerate walking, exercise, and rehab. Nutrition is rarely the only answer, but it can make the rest of the plan work better.
You probably won't need the same routine forever, but some ongoing movement work is usually wise. Think maintenance, not punishment. A few targeted exercises done consistently are often what helps preserve the gains you worked hard to build.
The strongest non-surgical plans usually combine core therapies rather than relying on one passive option. For many patients, that means a mix of pain relief, chiropractic care, spinal decompression, massage therapy, mobility therapy, rehabilitation exercise, and, when appropriate, muscle stimulation, acupuncture, or nutrition counseling. Patients with related issues such as sciatica treatment, post-injury care, or even movement restrictions found through a golf movement screening or car accident treatment evaluation may need the plan adapted to those findings.
If you're looking for a clear next step, Aspen Falls Wellness provides non-surgical musculoskeletal care in Salt Lake City and Sandy, including evaluation, chiropractic adjustment, DRX9000 spinal decompression, massage therapy, MLS Laser Therapy, SoftWave Therapy, mobility therapy, rehabilitation exercise, acupuncture, and nutrition counseling. The right plan starts with identifying what's driving your symptoms and building treatment in the right order.

Stay updated with the latest chiropractic news and exclusive offers.