Searching for a chiropractor for neck pain? Learn about evidence-based treatments like adjustments, decompression, and laser therapy in Salt Lake City & Sandy.
You wake up, roll to one side, and your neck reminds you first. It might be a sharp catch when you lift your head off the pillow. It might be a dull ache that spreads into your shoulder before coffee. By the time you sit at your desk, check your phone, or back the car out of the driveway, you're already moving cautiously.
That's where a lot of people start looking for a chiropractor for neck pain. Not because they want a dramatic fix, but because they're tired of guessing. They want to know what's causing the pain, what treatment makes sense, and whether there's a path forward that doesn't jump straight to medication or invasive care.
Good chiropractic care starts there. Not with a generic adjustment, but with a diagnosis-driven process that looks at joints, discs, nerves, muscle tension, posture, daily habits, old injuries, and how your symptoms behave over time.
Some people come in after a few days of stiffness. Others have been managing the same pattern for months. They've changed pillows, stretched in the shower, rubbed the sore spot between the neck and shoulder, and tried to avoid turning too fast. The pain eases for a day, then comes back.
That cycle trains people to lower their expectations. They stop asking, “Why does this keep happening?” and start saying, “Maybe this is just part of getting older,” or “Maybe I slept wrong again.” If that sounds familiar, a more useful next step is a real workup, not more trial and error. For readers dealing with recurring symptoms, this guide to chronic neck pain relief is a good place to start.
Neck pain rarely shows up without context. There's often a story behind it. Long hours with the head drifting forward over a laptop. A low-speed collision months ago that “wasn't that bad” until the stiffness never fully left. A gym strain. A disc issue that now refers pain into the shoulder blade or arm.
Practical rule: If your neck pain keeps returning, changes how you work, sleep, or drive, or starts radiating beyond the neck itself, it's time for a proper diagnosis.
A chiropractor for neck pain should help you answer three things. What tissue is irritated. Why it's being overloaded. What combination of treatment and home care gives it a chance to calm down and stay calm. That's very different from a quick crack-and-go approach.
The patients who do best usually follow a plan. Their care is adjusted to the cause of the problem, their exam findings, and how they respond over time. Some need gentle realignment and mobility work. Some need massage therapy and rehabilitation exercise because the muscles are guarding and the joints aren't moving well. Some need more advanced care because a disc or nerve is part of the picture.
The important point is simple. You don't have to just live with neck pain, and you shouldn't have to guess your way through it.
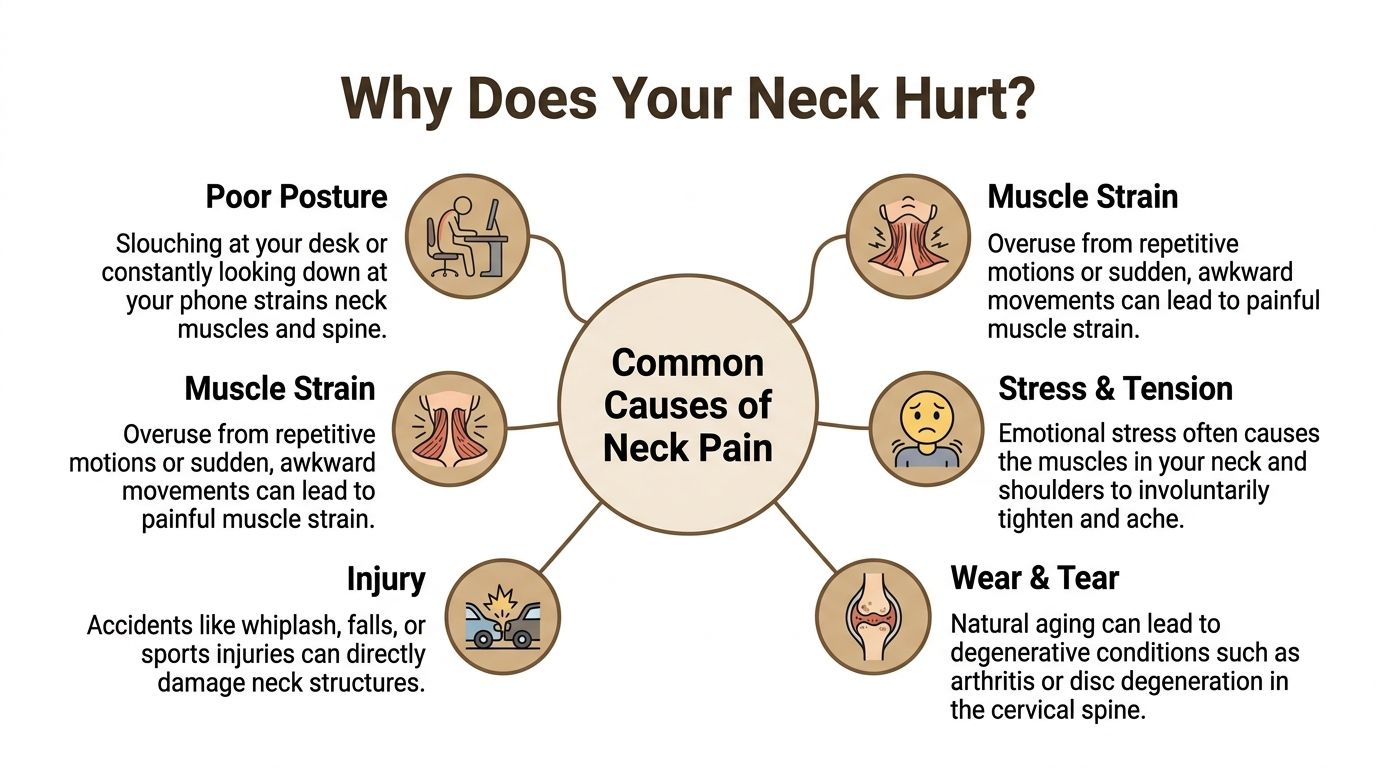
Most neck pain falls into a handful of patterns. The hard part is that different causes can feel similar at first. A tight, aching neck can come from posture, joint restriction, muscle strain, stress, a disc problem, or an old injury that never healed cleanly.
If you're trying to make sense of your own symptoms, it helps to think in categories instead of labels. This overview of neck pain conditions and treatment options can help you compare what you're feeling with common mechanical patterns.
Poor posture and tech neck: Your head is meant to balance over your shoulders. When it drifts forward for hours, the neck and upper back muscles have to hold that load all day. People often feel this as stiffness at the base of the neck, tension across the shoulders, or headaches that build later in the day.
Muscle strain: This can happen after repetitive work, yard work, travel, poor sleep position, or one awkward lift. The muscles tighten to protect the area, but then the guarding becomes part of the pain.
Stress-related tension: Emotional stress often shows up physically in the neck and shoulders. You may clench, raise your shoulders, or stay braced without realizing it. The result is soreness, reduced motion, and fatigue through the upper trapezius and base of the skull.
Injury and whiplash: Car accidents, sports impacts, and falls can strain ligaments, irritate joints, and create lingering movement problems. People sometimes underestimate these injuries because the pain doesn't peak until later.
Wear and tear: Arthritic change, disc degeneration, and chronic joint restriction can all contribute to recurring pain and reduced range of motion, especially if the supporting muscles have become weak or deconditioned.
Two people can both say, “My neck hurts when I turn left,” and need very different care. One may have a facet joint problem. Another may have a disc issue with referral into the arm. Another may have severe muscle guarding.
Current guidelines emphasize that practitioners must defer or modify procedures when vascular pathology is suspected, using history-led clinical reasoning rather than relying solely on pre-manipulative tests, a sophisticated safety standard that ensures patient safety before any treatment begins (vascular screening guidance for neck pain safety).
That point matters. Safe care starts before treatment. A careful history and targeted examination help identify who is a straightforward chiropractic case, who needs modified treatment, and who needs referral or imaging before anything else happens.
A first visit should feel thorough, not rushed. Patients commonly arrive with two concerns. They want pain relief, and they want to know whether the provider is listening. Both matter.

Before the exam begins, it helps to know what a new patient process looks like. This new patient information page gives a practical overview, but the short version is that the visit is built around history, physical findings, and a treatment plan that matches both.
The first conversation usually covers when the pain started, what makes it worse, whether it travels into the shoulder or arm, whether headaches are involved, and what daily tasks have become harder. A good history also includes old injuries, previous imaging, work demands, exercise habits, sleep position, and any numbness, tingling, weakness, or dizziness.
This part isn't small talk. It shapes the exam. If someone says their pain spikes after looking down, changes with coughing, or radiates below the shoulder, that points the workup in a different direction than pain that stays local and worsens only with muscular effort.
The exam usually includes:
A useful first visit doesn't end with “your neck is out.” It should end with a clear explanation of what was found, what likely caused it, and what the next step is.
Not every neck pain patient needs imaging. But sometimes X-rays or outside MRI referral are the right next step, especially when the history suggests trauma, nerve involvement, structural instability, or a condition that needs a closer look. The point isn't to image everyone. The point is to avoid guessing when the presentation calls for more information.
By the end of the visit, the treatment plan should make sense to you. You should know whether care will focus on chiropractic adjustment, mobilization, massage therapy, mobility therapy, rehabilitation exercise, muscle stimulation, or a more advanced option. You should also know what success looks like. Less pain is important, but so is sleeping better, turning your head while driving, working without a flare, and getting back to activity with confidence.
There isn't one single treatment that fixes every neck problem. That's why a good chiropractor for neck pain works from a toolkit, not a script. The right plan depends on whether the main issue is joint restriction, muscular overload, disc irritation, postural strain, accident-related injury, or a combination of several.
An adjustment can restore motion to a joint that isn't moving well. That's useful. But if the muscles around that joint are tight, weak, overworked, and retraining poor movement every day, the result often won't hold. The same is true in reverse. Stretching and rehab help, but they're harder to perform well if the joints remain stiff and painful.
Clinical guidelines explicitly recommend spinal manipulative therapy for chronic neck pain only when integrated with advice, exercise, mobilization, and soft-tissue therapy for both short- and long-term benefit in pain and disability, and the combination of manual therapy with active rehabilitative exercise significantly outperforms passive care alone (clinical guideline summary for multimodal neck pain care).
That matches what experienced clinicians see every week. The patients who maintain progress usually don't rely on a passive treatment alone. They pair hands-on care with movement correction, home exercise, and practical changes to work setup, training, and recovery habits.
| Therapy | Primary Goal | Best For |
|---|---|---|
| Chiropractic Adjustment | Restore joint motion and reduce mechanical irritation | Stiff, restricted segments and movement-related pain |
| Mobilization | Improve motion with a gentler, lower-force approach | Sensitive patients, guarded necks, or cases where manipulation isn't appropriate |
| Massage Therapy | Reduce muscle tension and soft-tissue restriction | Trigger points, stress tension, and postural overuse |
| MLS Laser Therapy | Support tissue recovery and calm irritated areas | Persistent soft-tissue pain and inflammatory presentations |
| Acupuncture | Modulate pain and reduce muscular guarding | Tension-driven pain and patients who respond well to neuromodulatory care |
| Muscle Stimulation | Help relax overactive muscles and support pain relief | Acute spasm and protective guarding |
| Mobility Therapy | Improve usable range of motion | Stiff necks that have lost smooth, confident movement |
| Rehabilitation Exercise | Build strength, endurance, and movement control | Recurrent pain, posture-related pain, and long-term prevention |
| Personal Exercise Plans | Extend treatment into daily life | Patients who need a realistic home program |
| Nutrition and Nutrition Counseling | Support recovery habits and inflammation management | Patients whose healing is affected by broader health factors |
For many people, the most effective plan combines several tools in a specific order. A visit might start with soft-tissue work or massage therapy to reduce guarding. Then a chiropractic adjustment or mobilization restores motion more comfortably. Laser, acupuncture, or muscle stimulation may help settle irritated tissue. Corrective exercise then teaches the body how to hold that improvement.
A multimodal approach combining spinal manipulative therapy with stretching, strengthening, and endurance exercises is strongly recommended for chronic neck pain, and retrospective outcome analyses cited in that literature report that approximately 57% of patients had at least a 75% reduction in pain after 12 weeks, compared with 33% in medication-only groups (multimodal neck pain evidence overview).
If a treatment helps for a day but the pain returns with the same tasks, the plan probably needs more than symptom relief. It needs capacity building.
That's why realignment alone isn't the whole answer for chronic cases. Long-term change usually comes from combining pain relief with retraining. In practical terms, that may mean posture work for office users, rehabilitation exercise for athletes, mobility therapy for restricted upper backs, or car accident treatment after whiplash when the neck and shoulder complex has lost normal movement patterns.
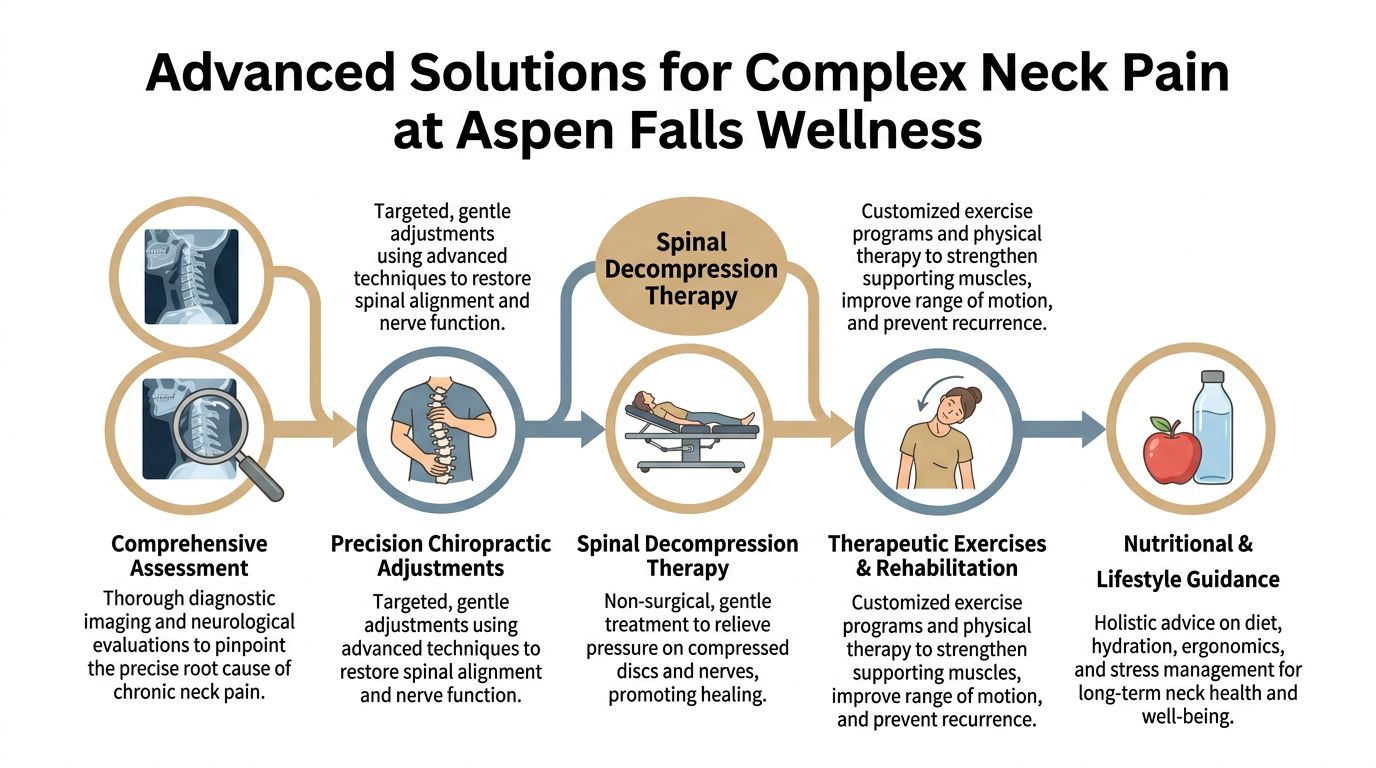
One example of this integrated model is Aspen Falls Wellness, where care may combine chiropractic adjustment, spinal decompression, MLS Laser Therapy, massage therapy, acupuncture, mobility therapy, and take-home exercise based on the diagnosis rather than a one-size-fits-all schedule.
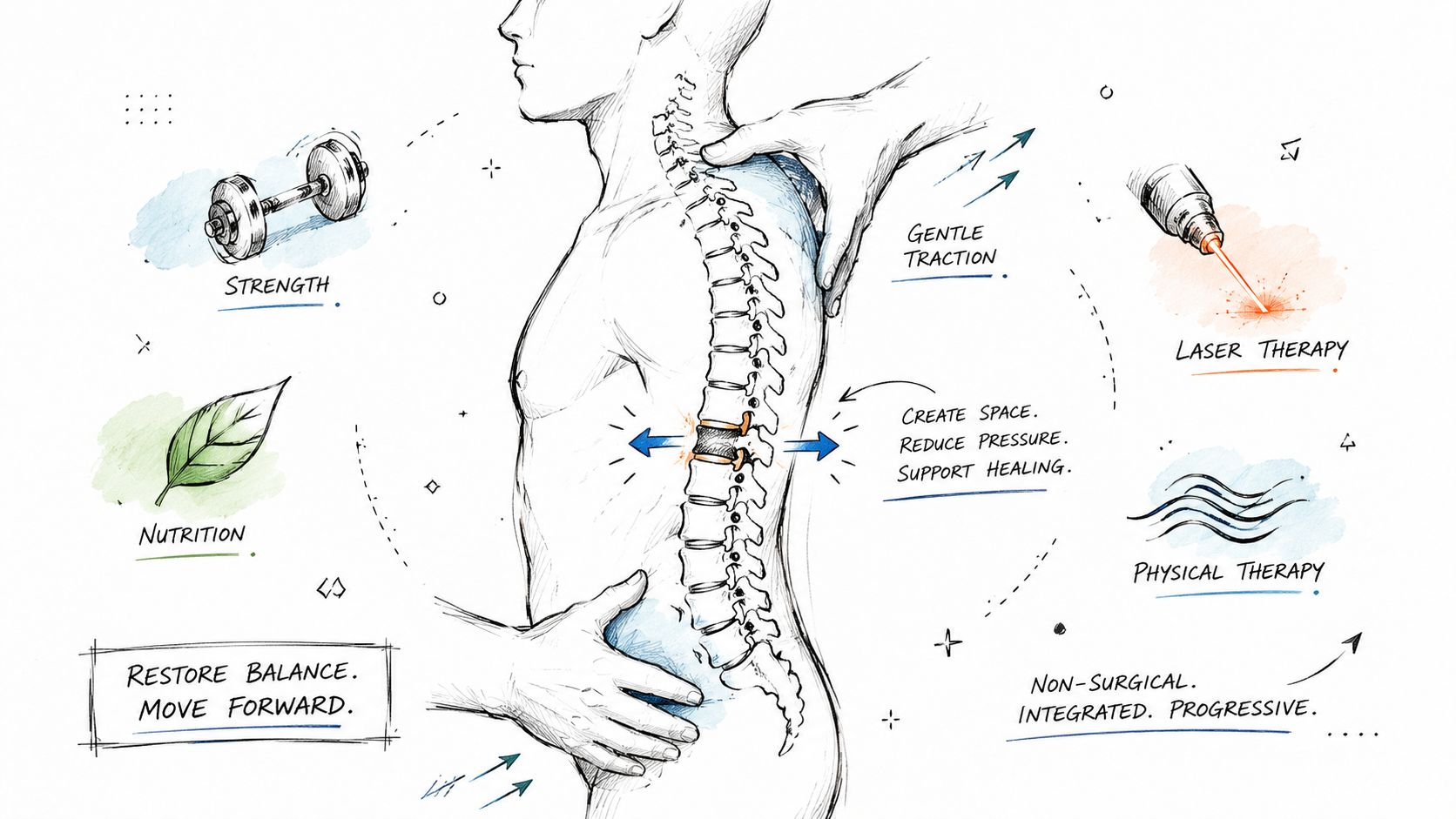
Some neck pain isn't simple. The patient isn't just stiff. They're dealing with recurring flare-ups, arm symptoms, disc involvement, or pain that hasn't responded to basic conservative care. That's where advanced options can become useful, especially when they're applied as part of a broader plan rather than as standalone technology.
Spinal decompression is most relevant when disc mechanics and nerve pressure are part of the problem. In those cases, ordinary stretching often isn't precise enough, and generic traction may not create a consistent therapeutic effect. Computer-controlled decompression is designed to apply a measured pull that reduces pressure and supports healing conditions around the affected disc.
For disc-related spine conditions, a retrospective chart audit of 94 outpatients treated with the DRX9000 reported a mean 83% improvement in pain after an average follow-up of 31 weeks, with a post-treatment Numeric Rating Scale score of 1.7 and a patient satisfaction score of 8.55 out of 10 (DRX9000 outcome summary). That specific data comes from low back pain and sciatica cases rather than neck pain cases, but it helps explain why decompression remains part of the conversation when disc pathology drives symptoms elsewhere in the spine.
There's also an important financial trade-off. While the DRX9000 is FDA-cleared and shows high success rates, major insurance policies including Aetna often classify spinal decompression as “experimental” and may not provide coverage, which is why many patients pay out-of-pocket for this effective treatment (insurance and coverage reporting on spinal decompression).
Advanced care shouldn't replace clinical reasoning. It should support it.
The more complex the case, the more important sequencing becomes. Calm the irritated tissue first. Restore motion second. Rebuild function third.
For neck pain specifically, high-force treatment isn't always the right choice. Evidence from the UCLA Neck-Pain Study found that cervical mobilization yields clinically equivalent outcomes to manipulation for reducing pain severity and disability after 6 months, with a significantly lower risk of serious adverse events, and adding heat or electrical muscle stimulation didn't appreciably improve long-term outcomes (UCLA Neck-Pain Study summary). That's why complex neck cases often benefit from a more selective approach. Less force, better targeting, and more support work around the treatment itself.
If you're searching for a chiropractor for neck pain in Salt Lake City, ask better questions than “Do they do adjustments?” Almost everyone does. The more useful question is whether they can diagnose the problem accurately and build a plan around it.
Start with the basics. Ask how they evaluate neck pain, when they refer for imaging, and how they decide between adjustment, mobilization, massage therapy, rehabilitation exercise, acupuncture, or decompression. Ask how progress is measured. A solid clinic should be able to explain what changes they expect to see in pain, motion, function, and daily tolerance.
There's also a broader value question. In a comparative effectiveness analysis, chiropractic physician care for neck pain reduced total per-patient spending by $302 annually compared to medical physician care. That doesn't mean every clinic is equal. It does mean conservative chiropractic management can make sense clinically and financially when it's done well.
If you're researching local providers online, it also helps to understand how clinics present themselves in search results and maps. This guide to mastering local search for chiropractors offers a practical look at the signals that influence local visibility, which can help patients evaluate why certain practices appear more prominently and how to vet them beyond rankings.
Neck pain usually doesn't improve for long because of one perfect treatment. It improves when the underlying driver is identified and the plan matches it. For some people that means chiropractic adjustment and mobility therapy. For others it means massage, acupuncture, laser, decompression, or a stronger home exercise plan. Most chronic cases need a combination.
A good first step is to pay attention to your pattern. Notice when the pain starts, where it travels, what positions aggravate it, and what time of day it's worst. Bring that information with you. It often shortens the path to a clear diagnosis.
Relief is possible, but the plan has to fit the problem.
If you've been hoping the pain will fade on its own, or if treatment elsewhere has only helped briefly, getting answers is the next move. You don't need to commit to a lifetime plan. You need a diagnosis, a realistic treatment strategy, and a provider who can explain the trade-offs clearly.
If you're ready to get clear on what's causing your neck pain and what non-surgical options make sense, contact Aspen Falls Wellness to schedule a thorough consultation in Salt Lake City or Sandy. The goal is straightforward: identify the source of the problem, match treatment to the diagnosis, and build a practical plan for lasting pain relief.

Stay updated with the latest chiropractic news and exclusive offers.