Find lasting chronic neck pain relief with this step-by-step guide. Learn at-home exercises, posture fixes, and when to seek advanced care in Salt Lake City.
You wake up, turn your head toward the alarm, and feel that familiar pull from the base of your skull into your upper shoulder. By mid-morning, the stiffness has turned into a dull ache. By afternoon, you're shifting in your chair, rubbing the same spot, and wondering why a simple workday feels like a physical test.
That pattern wears people down. Chronic neck pain doesn't just hurt. It changes how you sleep, how you drive, how long you can focus, and how much patience you have left by the end of the day. The good news is that lasting chronic neck pain relief usually doesn't come from one magic fix. It comes from making the right decision at the right stage, starting with smart self-care and escalating only when your symptoms and exam findings justify it.
You wake up and turn your head toward the nightstand, and that sharp, familiar pull is back. A hot shower loosens it enough to get moving. By midafternoon, after a few hours at a desk or in the car, the stiffness builds again, the upper shoulders tighten, and even checking a blind spot feels like work.
Chronic neck pain means pain lasting three months or longer, and it affects approximately 2.2% of the general U.S. population as chronic impairing pain, according to this review in PMC. The true burden is not merely the pain itself. It is the way pain starts organizing your day around what you avoid, cut short, or push through.
Sleep often suffers first. One awkward position can wake you up, and a restless night lowers your tolerance the next day. Then simple tasks start to stack up. Computer work, carrying a bag, workouts, yard work, long drives, even relaxing on the couch can all become small tests of what your neck will allow.
A common approach is to manage it with medication. That same review found that 56.3% of people with chronic impairing neck pain use over-the-counter NSAIDs, while 29% use strong narcotics. Medication can reduce pain enough to get through the day, and in the right situation that matters. The trade-off is that it usually does not correct the joint stiffness, muscle guarding, disc irritation, posture stress, or movement habits that keep the cycle going.
In clinic, chronic neck pain rarely looks random. It follows patterns. Position matters. Load matters. Sleep, stress, work setup, and how often you move all matter.
That is why short-term relief and long-term recovery need different decisions. Some flare-ups respond well to a few days of smart home care. Some patterns keep returning because the underlying problem has not been identified or because home care is no longer enough. If you are trying to sort out where your symptoms fit, this guide to common types of neck pain and what they can mean can help you frame the next step.
A better plan usually works in stages:
That progression gives you a practical way to choose what to do next, instead of treating each painful day like a separate problem.
Not all neck pain comes from the same place. Some people have irritated joints that don't glide well. Others have overloaded muscles around the neck and shoulder blade. Some have disc-related pain, whiplash-related dysfunction after a car accident, or a nervous system that keeps amplifying symptoms after tissues should have calmed down.
One of the biggest modern drivers is tech neck, but that phrase gets oversimplified. It isn't just slouching over a phone. According to UT Southwestern's discussion of tech neck pain treatments, chronic forward-head posture can alter pain signaling and neuromuscular function, and 14% of cases persist beyond 6 months due to unaddressed neuro-muscular changes. That's why “sit up straight” often doesn't fix a problem that's been building for months.

A useful way to think about causes is this:
| Source | What it often feels like | Why it keeps returning |
|---|---|---|
| Joint restriction | Pinching, stiffness, pain with turning | The segment never regains smooth motion |
| Muscle overload | Tight bands, upper trap burning, tension headaches | Weak support muscles force larger muscles to overwork |
| Disc or nerve irritation | Neck pain with radiating symptoms, guarding, pain with load | Mechanical pressure and inflammation aren't fully reduced |
| Postural adaptation | Ache after screens, rounded shoulders, chin-forward position | Daily habits reinforce the same strain pattern |
| Sensitized pain system | Pain feels bigger than the movement should cause | The nervous system stays on high alert |
If you're trying to sort out your own pattern, a focused neck pain evaluation should look at posture, movement quality, neurological signs, work habits, sleep setup, and symptom triggers. The exact tissue matters less than the pattern at first. The pattern tells you which level of care makes sense.
Practical rule: If your pain is always linked to the same positions or tasks, there's usually a modifiable mechanical driver. If symptoms are unpredictable, spreading, or escalating, the exam matters even more.
Most chronic neck pain is mechanical and treatable without surgery. Some symptoms need prompt medical evaluation and shouldn't be managed with home exercises alone.
Watch for these red flags:
Those signs don't automatically mean something severe is happening. They do mean you shouldn't guess.
When your neck flares up, the goal is simple. Reduce irritation without teaching your body to stiffen around it. Too much rest can backfire. Too much stretching can also backfire. The sweet spot is calm, supported movement.
Start with a short relief sequence instead of random trial and error:
Common self-treatments are popular, but they aren't all equally helpful. Earlier evidence has noted heavy use of heat, cold, and electrical stimulation, while benefit is often unclear or limited. That's why I prefer using them as support tools, not the center of the plan.
If your flare-up comes with a headache, some people also like simple, low-risk comfort measures such as natural headache relief with peppermint oil, especially when combined with hydration, reduced screen exposure, and neck unloading.
For muscle-driven flare-ups, hands-on soft tissue care can help break the cycle of guarding. If that pattern sounds familiar, massage therapy for neck and shoulder tension can complement your home plan rather than replace it.
Sleep is where many good treatment plans fall apart. A recent analysis reported that 31% of neck pain patients experience a high rate of recurrence, often tied to unaddressed micro-strains during sleep, and emphasized that sleep posture is a measurable clinical variable in neck pain care (PMC analysis on sleep posture and recurrence).
That means your pillow setup isn't a comfort detail. It's part of treatment.
Use these sleep rules:
If you feel better as the day goes on but wake up stiff every morning, don't ignore your sleep setup. It may be re-irritating the same tissues every night.
If you want long-term chronic neck pain relief, exercise can't be an afterthought. It's the anchor. A JOSPT review on neck pain rehabilitation reported that exercise has the strongest evidence-based treatment effect for chronic neck pain, and a 2018 systematic review concluded it can reduce the risk of a new episode by 53%.
That doesn't mean random internet stretches. It means a program that restores support, control, and movement quality.
Attempting to “fix posture” often involves forcing oneself upright. That usually creates more tension in the upper traps and lower back. Better posture comes from better support.
Focus on three pillars:
Here's the trade-off. Stretching tight areas can feel good quickly, but without strengthening the weak links, the tightness usually returns. Strength work is slower to pay off, but it changes the pattern.
A practical home program doesn't need to be complicated. It needs to be repeatable.
Consider this structure:
A sample posture snack might look like this:
| Time | Reset |
|---|---|
| After long screen work | Stand, walk, reset shoulder blades, loosen jaw |
| After driving | Gentle neck turns and chest opening |
| Mid-afternoon slump | Chin tuck control plus upper back extension |
The right amount matters. If exercises leave you sharply worse for the rest of the day, back off. If they create mild effort and better motion afterward, you're usually in the right zone.
Key takeaway: The best neck program doesn't chase fatigue. It teaches your neck and shoulder girdle to share load correctly again.
This is also where personal exercise plans, mobility therapy, and rehabilitation exercise become more than service labels. They matter because the exact mix should match your pattern. A sedentary office worker with tech-neck mechanics needs a different plan than someone recovering from a car accident, a golfer trying to regain rotation, or a patient with disc irritation who can't tolerate aggressive loading yet.
You wake up with the same neck pain again. The heat helped last night. The stretches gave you a short window of relief. By lunch, your neck is tight, your head feels heavy, and turning to check traffic is back to being a chore.
That pattern usually means home care has taken you as far as it can on its own. The next step is not more random treatment. It is a better diagnosis and a plan that matches the primary driver of your symptoms.
A few warning signs matter more than the pain score itself. Pay attention if your symptoms keep returning after brief relief, your range of motion is getting worse, or the pain is spreading into the shoulders, shoulder blade, or arm. Those patterns can point to joint restriction, irritated soft tissue, disc involvement, nerve sensitivity, or a combination.
Exercise tolerance is another decision point. If gentle progression leaves you moderately sore but looser later, that is often acceptable. If each attempt to strengthen or mobilize your neck sets off a flare that derails the rest of your day, you need a closer look.
Daily function matters too. Trouble sleeping, driving, working at a screen, lifting, or concentrating because of persistent pain tells me the problem is affecting more than one part of your life. At that stage, waiting it out often prolongs the cycle.
A useful exam should change the treatment plan. It should sort out whether the main issue is mechanical, inflammatory, nerve-related, postural, or load-related, then build care around that finding.
In practice, that often means combining several approaches instead of repeating one treatment that gives only temporary relief:
The trade-off is straightforward. Passive care can reduce pain faster. Active care usually makes results last longer. Chronic cases tend to need both, in the right order.
One example is the office worker whose neck pain comes with headaches by midweek. Restoring joint motion may help first. Reducing muscle guarding may make movement easier. Then targeted rehab can improve deep neck control and shoulder blade support so the same workday posture stops recreating the problem. If irritability stays high, adding a modality to calm the area may make exercise tolerable again.
At Aspen Falls Wellness, the value of personal exercise plans, mobility therapy, chiropractic care, massage therapy, acupuncture, and advanced device-based options comes from matching each one to a specific barrier in recovery. Intake also matters. Good clinics need a clear symptom history, aggravating factors, prior imaging, and functional limits before treatment starts. Formzz's guide to patient intake gives a useful look at how structured intake improves that process.
A better question than “Which treatment is best?” is “What is blocking progress right now, and what care is most likely to remove that block?”
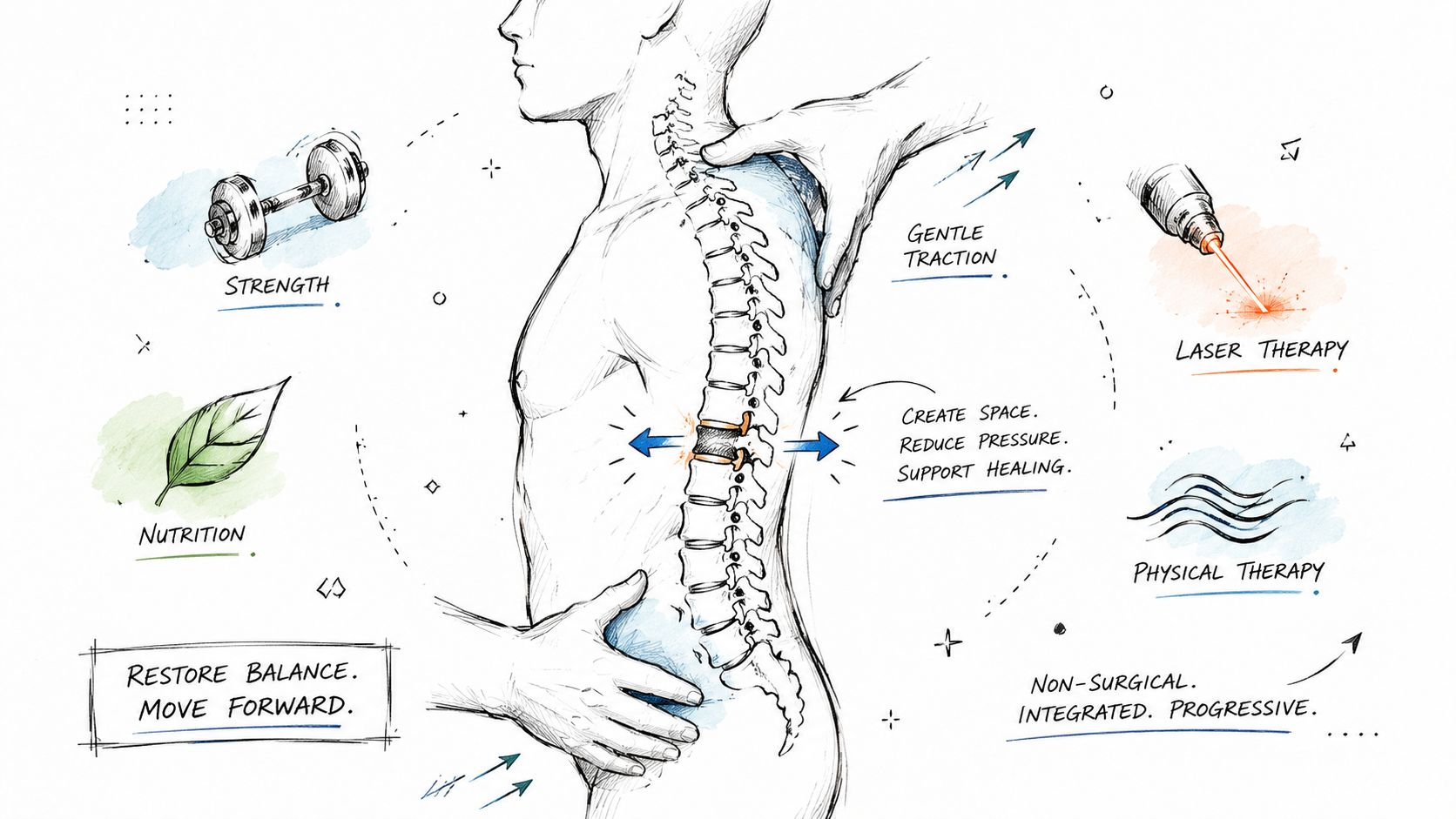
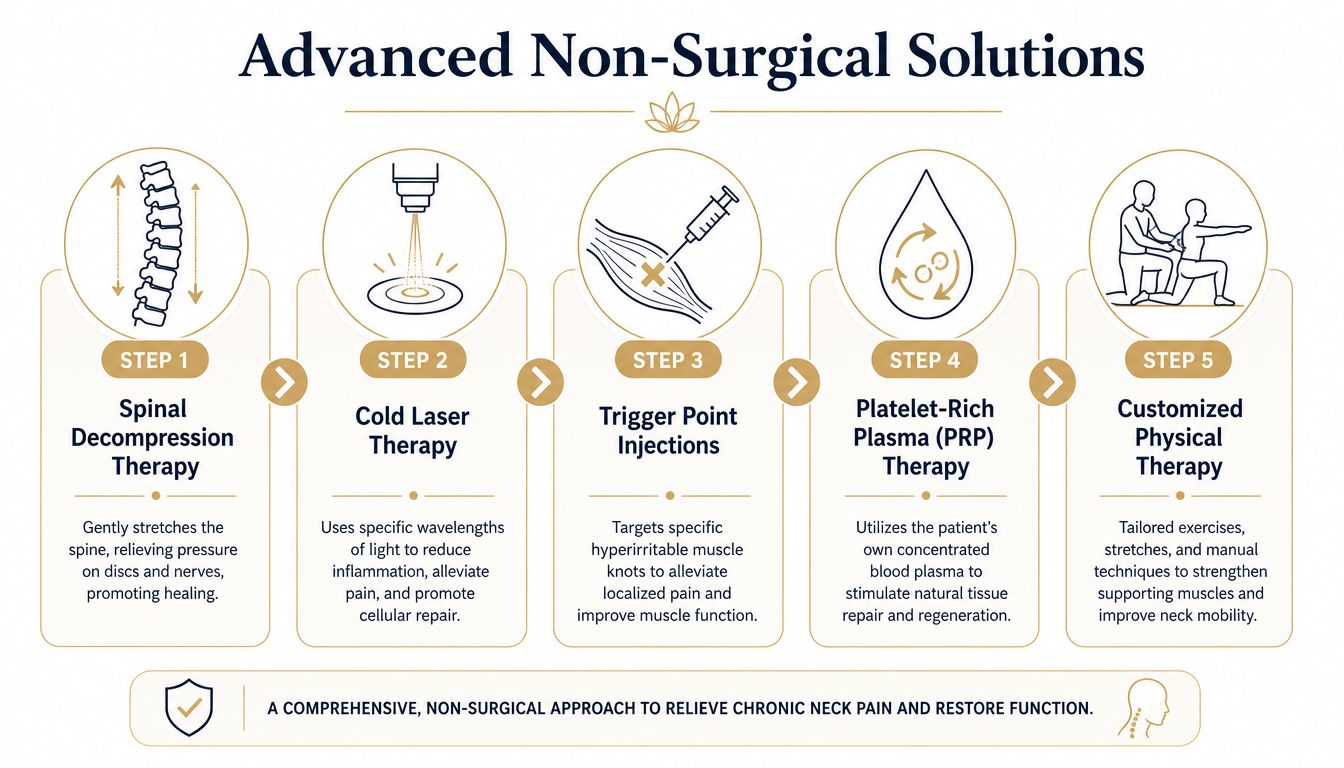
Some cases don't resolve with adjustments, exercise, and soft tissue work alone. That's especially true when disc involvement, nerve irritation, or persistent mechanical compression keeps re-triggering symptoms. In those situations, advanced non-surgical care can create room for healing without jumping straight to invasive procedures.

Spinal decompression is one of the more useful options when symptoms suggest disc and nerve pressure are part of the problem. The DRX 9000 is an FDA-cleared powered traction device designed to apply precisely controlled decompression forces, typically across about 20 sessions over 4 to 6 weeks, with sessions lasting 30 to 45 minutes, according to this overview of DRX9000 spinal decompression.
There's also a published case series in lumbar intervertebral disc lesions showing that non-surgical spinal decompression with the DRX9000 produced an 80% reduction in pain after 20 treatments and a 50% improvement in disability scores (clinical case series on DRX9000 outcomes). That study is on lumbar patients, so it shouldn't be overstated as a neck-specific promise. But it does help explain why decompression remains part of the conversation for disc-related spine care.
The basic idea is straightforward. Controlled traction reduces pressure around discs and irritated nerve structures. In the right patient, that can lower pain enough to let movement retraining, strengthening, and normal daily function return.
If you want a deeper overview of how this approach is used in practice, spinal decompression therapy for disc-related pain is worth reviewing before an exam.
Decompression isn't the only advanced option, and it isn't right for every case.
MLS Laser Therapy is often used when inflammation and tissue irritability are keeping progress stuck. In clinic, the practical goal is to reduce pain enough that the patient can tolerate corrective exercise, posture retraining, and normal daily loading again.
SoftWave Therapy can support tissue stimulation and healing in stubborn soft-tissue presentations. It may be considered when a patient has chronic myofascial pain, persistent attachment-point tenderness, or symptoms that haven't improved enough with manual care and exercise alone.
Some patients also need a calmer bridge into active care. That's where massage therapy, muscle stimulation, acupuncture, or carefully dosed adjustment can help. These aren't stand-alone cures for a chronic pattern. They can, however, lower the barrier to effective rehabilitation.
A practical way to think about advanced care is by obstacle:
| Main obstacle | Tool that may help |
|---|---|
| Disc and nerve pressure pattern | DRX 9000 spinal decompression |
| Inflamed, irritable tissue | MLS Laser Therapy |
| Stubborn soft tissue dysfunction | SoftWave Therapy or Massage Therapy |
| Pain-sensitive nervous system | Acupuncture plus graded exercise |
| Poor movement carryover | Personal Exercise Plans and Rehabilitation Exercise |
For clinics, a smooth intake process also matters more than people realize. If you're comparing what a thorough onboarding workflow should look like, Formzz's guide to patient intake gives a useful general look at how structured intake improves clarity before treatment even starts.
A reasonable escalation path usually looks like this:
The biggest mistake is waiting until pain controls your routines before getting a proper exam. The second biggest mistake is escalating too fast without giving active rehab a fair chance.
If you're looking for a structured path to chronic neck pain relief, Aspen Falls Wellness offers non-surgical care that can move from exam and conservative treatment to advanced options like spinal decompression, SoftWave Therapy, MLS Laser Therapy, massage, acupuncture, and rehabilitation exercise when clinically appropriate.

Stay updated with the latest chiropractic news and exclusive offers.