
Explore spinal decompression therapy, a non-surgical treatment for back pain. Learn how it works, who it helps, and how it fits into an integrated care plan.
If you're reading this while shifting in your chair, standing up every few minutes, or wondering whether this back and leg pain is going to turn into surgery, you're not alone. Individuals exploring spinal decompression therapy have often already attempted various treatments. Rest. Stretching. Medication. Maybe chiropractic care, massage therapy, or generic exercise handouts. Some improve for a bit, then the pain returns the moment they sit too long, drive, bend, or try to get back to normal life.
That's where a clearer conversation helps. Spinal decompression therapy can be a very useful non-surgical option for the right patient, especially when disc-related pressure is part of the problem. But it's not magic, and it shouldn't be sold that way. The honest clinical view is simpler: decompression can reduce pressure on irritated spinal structures, create a better environment for healing, and make it easier for a patient to progress into the active work that helps results last.
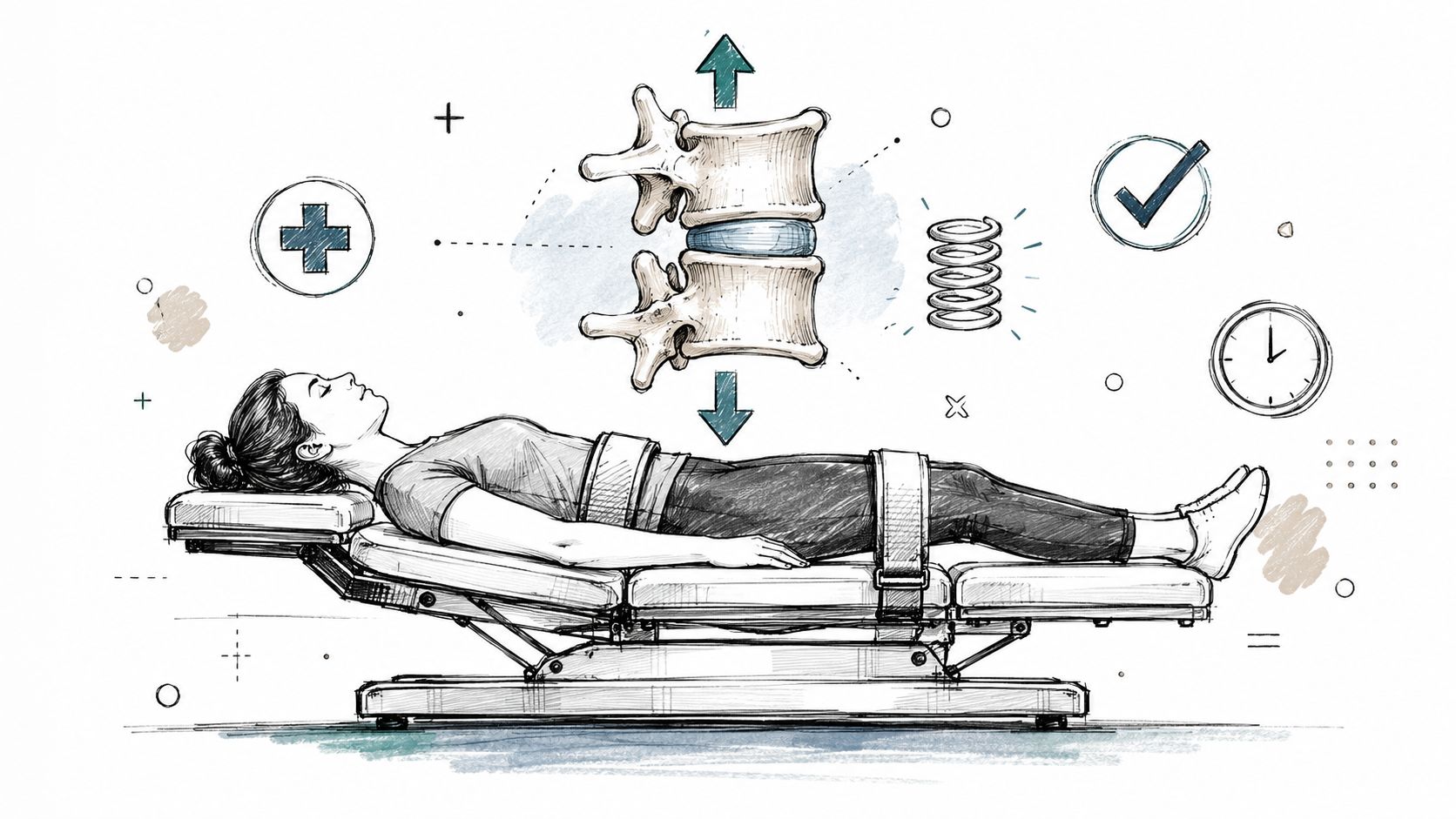
Think of a compressed spring. When pressure keeps pushing down on it, the coils lose space. If you apply the right amount of controlled tension, the spring opens gradually instead of snapping. That's the simplest way to understand spinal decompression therapy.
A painful lumbar disc often behaves the same way. The disc sits between vertebrae and can become irritated, bulged, or herniated. When that happens, nearby nerves can get crowded. The goal of decompression isn't to yank the spine. It's to create a controlled reduction in pressure so the disc has room to respond.
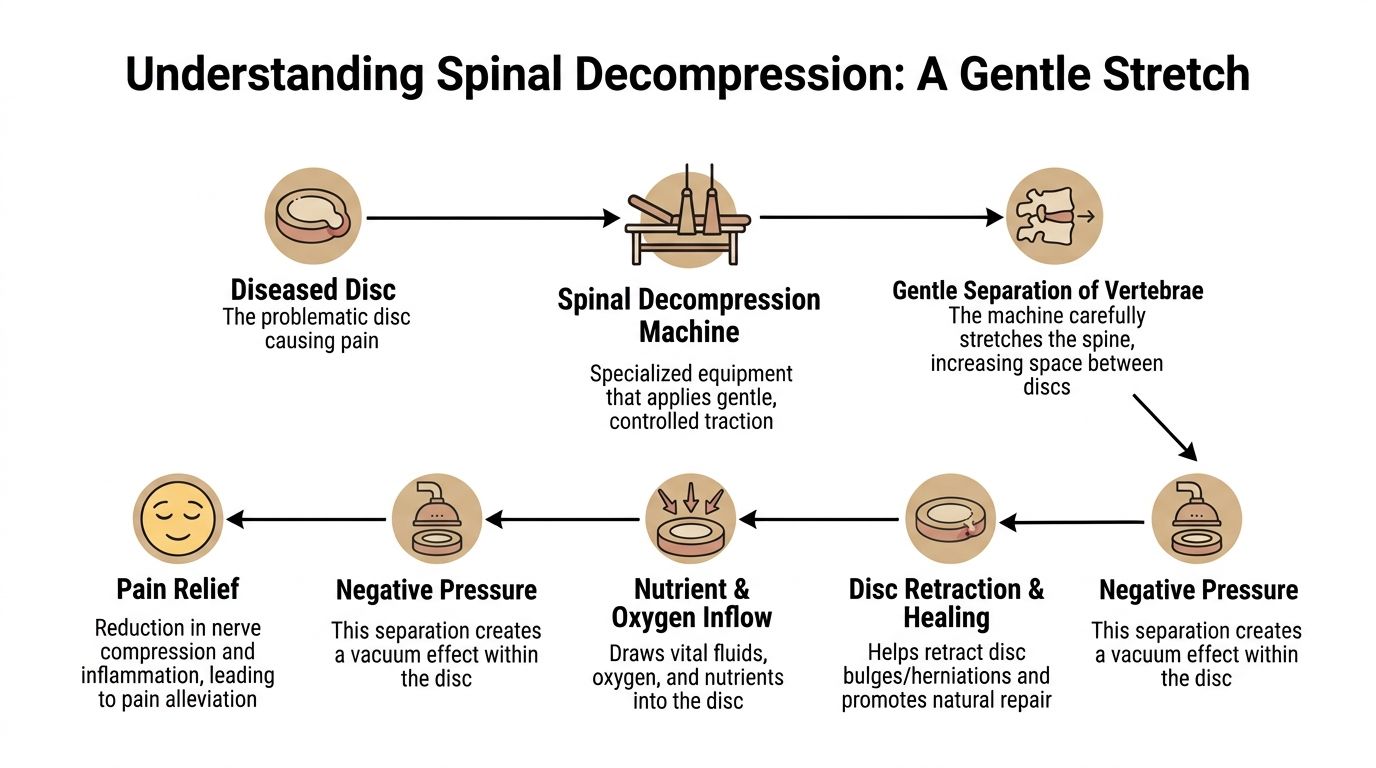
The DRX9000 is designed to apply a specific pull pattern rather than simple straight traction. According to the FDA-cleared device documentation for the DRX9000, the system achieves decompression by applying logarithmic distraction tensions that precisely elongate the spine. That process creates biochemical and biomechanical changes that help reposition displaced disc material and stimulate cartilage regeneration, with zero reported device-related injuries over twelve years in clinic monitoring.
That wording matters. Standard traction pulls. Decompression aims to target spinal structures in a more precise, computer-controlled way.
When vertebrae separate in a controlled manner, pressure inside the disc can drop. That's the effect clinicians often describe as negative intradiscal pressure. In practical terms, that can help with three things:
A good decompression session should feel controlled and specific. It shouldn't feel like someone is forcing your spine.
If you're the kind of patient who wants to understand the anatomy before starting care, these top anatomy learning tools can make the structure of discs, nerves, and vertebrae much easier to visualize.
Decompression creates an opportunity. It doesn't automatically build stability, restore movement habits, or correct the muscular patterns that helped create the problem. That's why some people feel temporary relief from passive care but don't hold their gains. The decompression table can lower the pressure. Your body still needs support to use that window well.
Some patients are strong candidates for spinal decompression therapy. Others shouldn't do it at all. The difference comes down to diagnosis, not how severe the pain feels on a bad day.
Decompression usually makes the most sense when symptoms point to disc-related compression. That often includes:
The DRX9000 is FDA-cleared for herniated discs, bulging discs, degenerative disc disease, and posterior facet syndrome in the context of low back pain management, which gives a reasonable framework for who may benefit when the exam matches the history.
This is where honest screening matters. A patient with severe nerve compromise, major instability, fracture, infection, or another condition outside conservative care needs a different plan. Decompression also isn't appropriate for some people with pregnancy, spinal fusion hardware, or severe osteoporosis.
A few practical red flags deserve immediate medical evaluation before any conservative plan:
Practical rule: If symptoms suggest a structural emergency, don't start with decompression. Start with the right medical workup.
A consult is worth considering if most of these sound familiar:
| Pattern | More likely to fit decompression |
|---|---|
| Pain behavior | Worse with sitting, bending, lifting, or driving |
| Leg symptoms | Tingling, numbness, burning, or radiating pain |
| Previous care | Some temporary relief, but symptoms keep returning |
| Goal | Avoid surgery if possible and improve function |
Patients with spinal stenosis often ask whether decompression can still help. The answer depends on the exact anatomy, severity, and overall exam findings. For a broader look at conservative options, this discussion of stenosis treatment without surgery is useful context.
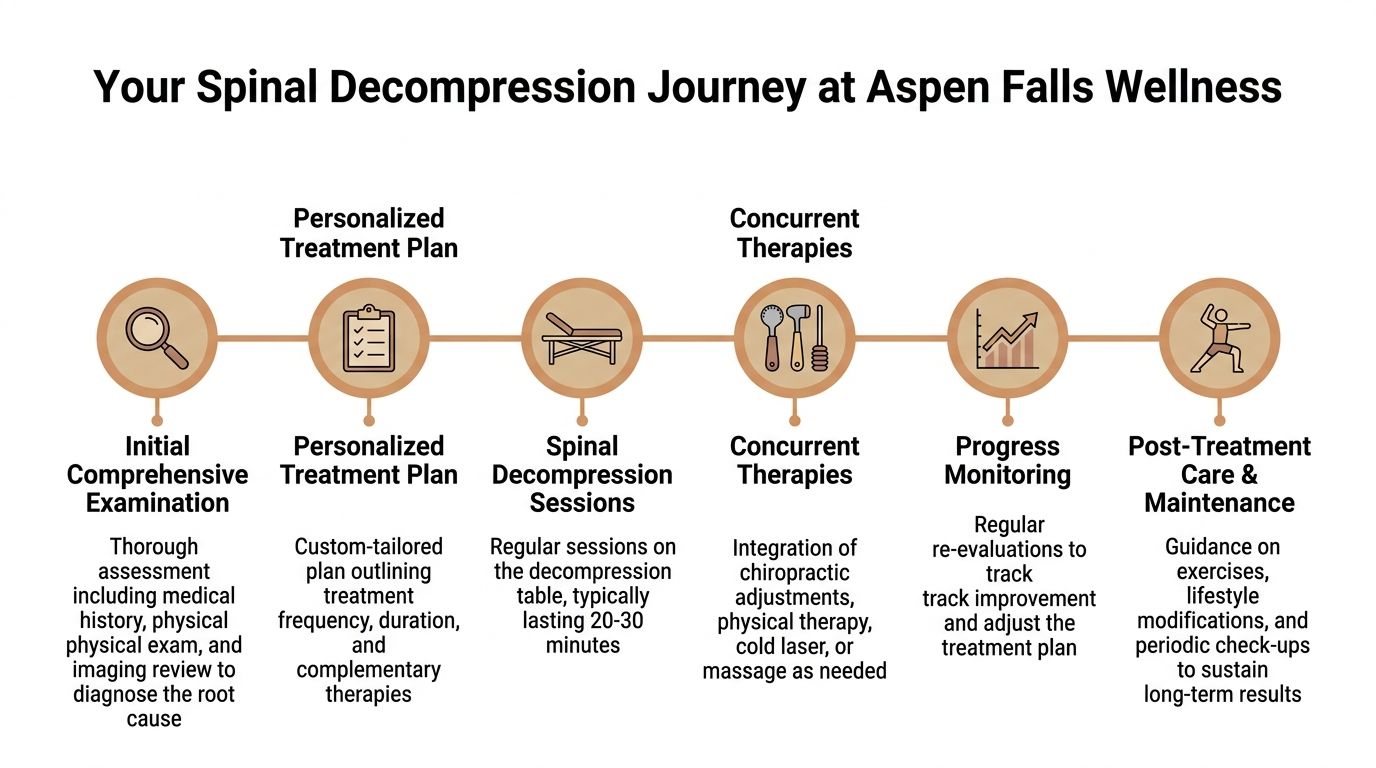
The treatment course starts long before the first pull on the table. The initial step is diagnosis. If someone has low back pain from a disc problem, decompression may be appropriate. If the same symptom pattern is being driven by another issue, the machine won't solve the wrong problem.
A proper workup includes history, movement testing, orthopedic examination, neurological screening, and imaging review when available. That's how a clinician decides whether decompression, chiropractic adjustment, rehabilitation exercise, muscle stimulation, MLS Laser Therapy, massage therapy, acupuncture, mobility therapy, or referral out makes the most sense.
Once the case fits, the schedule becomes fairly structured. A standard DRX9000 protocol involves 20 to 24 sessions, each lasting about 30 minutes, typically scheduled five times weekly for the first two weeks, three times weekly for the next two, and twice weekly for the final two weeks to support consistent decompressive force and therapeutic benefit, according to the DRX9000 protocol overview.
Most patients describe the session as an intermittent, gentle stretch. You're secured with harnessing so the force is directed where it needs to go. The table cycles through pull and partial relaxation phases. That rhythm matters because it helps the body tolerate the treatment without tightening against it.
What you should feel:
What you shouldn't feel:
Computer-assisted emergency stop switches are part of the device setup, which helps make the process feel safer for patients who are anxious about being on a traction-style table.
The people who do best usually don't treat decompression like an isolated event. They move carefully between visits, follow home guidance, and progress into corrective work as symptoms allow. That's also why this overview of DRX 9000 spinal decompression is helpful. It frames the machine as part of a care pathway, not the whole pathway.
Relief during the first week is encouraging. Relief that holds between visits is more meaningful.
Patients deserve a direct answer to the question that matters most. Does it work? The evidence is encouraging for disc-related cases, but it's important to stay precise about what the research does and doesn't say.
For patients with herniated discs, one of the more frequently cited outcome reports is notably positive.
According to Orthopedic Technology Review findings summarized here, non-surgical spinal decompression showed an 86% success rate for patients with herniated discs. In that same report, 92% showed significant improvement, and 89% maintained benefits 90 days after treatment ended.
That's clinically meaningful because it speaks to more than momentary pain relief. It suggests many patients improved and held their gains for a defined period after care.
The roots of modern mechanical decompression go back to the DRS Mechanical Decompression Distraction System introduced and clinically validated in 1998 by C. Norman Shealy, MD, PhD, and Borgmeyer. In that outcome study, spinal decompression was effective in 71% of cases, with pain levels dropping to 0 or 1 on a 0-to-5 scale. In a four-year follow-up of 23 responsive patients, 52% reported a pain level of zero, 91% resumed normal daily activities, and over 80% had at least a 50% reduction in pain at the end of that period, according to the 1998 decompression therapy research PDF.
That long-term follow-up is worth noting because spine patients often fear temporary results. Durable function matters more than a short-lived pain drop.
Other published material remains favorable for selected disc cases.
A case series on DRX9000-based non-surgical spinal decompression reported an 80% reduction in pain, a 50% improvement in disability scores, and a 75% subjective improvement in activities of daily living, along with MRI evidence of increased disc height and anterior-posterior dimension in the Parker journal case series.
There are also reports of success rates between 71% and 89% for disc-related conditions, including a study reporting an 88.9% success rate after a six-week DRX9000 protocol for neck and back pain, as summarized in this review of spinal decompression therapy outcomes.
The most important limitation is comparative evidence. Positive decompression outcomes are not the same as proof that decompression is better than every other conservative option for every patient. That nuance matters, especially when clinics market passive care as if it replaces active rehabilitation.
Most people weighing decompression are also thinking about surgery, chiropractic adjustments, physical therapy, or just waiting and hoping the flare settles. Each path has trade-offs. The right choice depends on diagnosis, severity, goals, and how your body has responded so far.
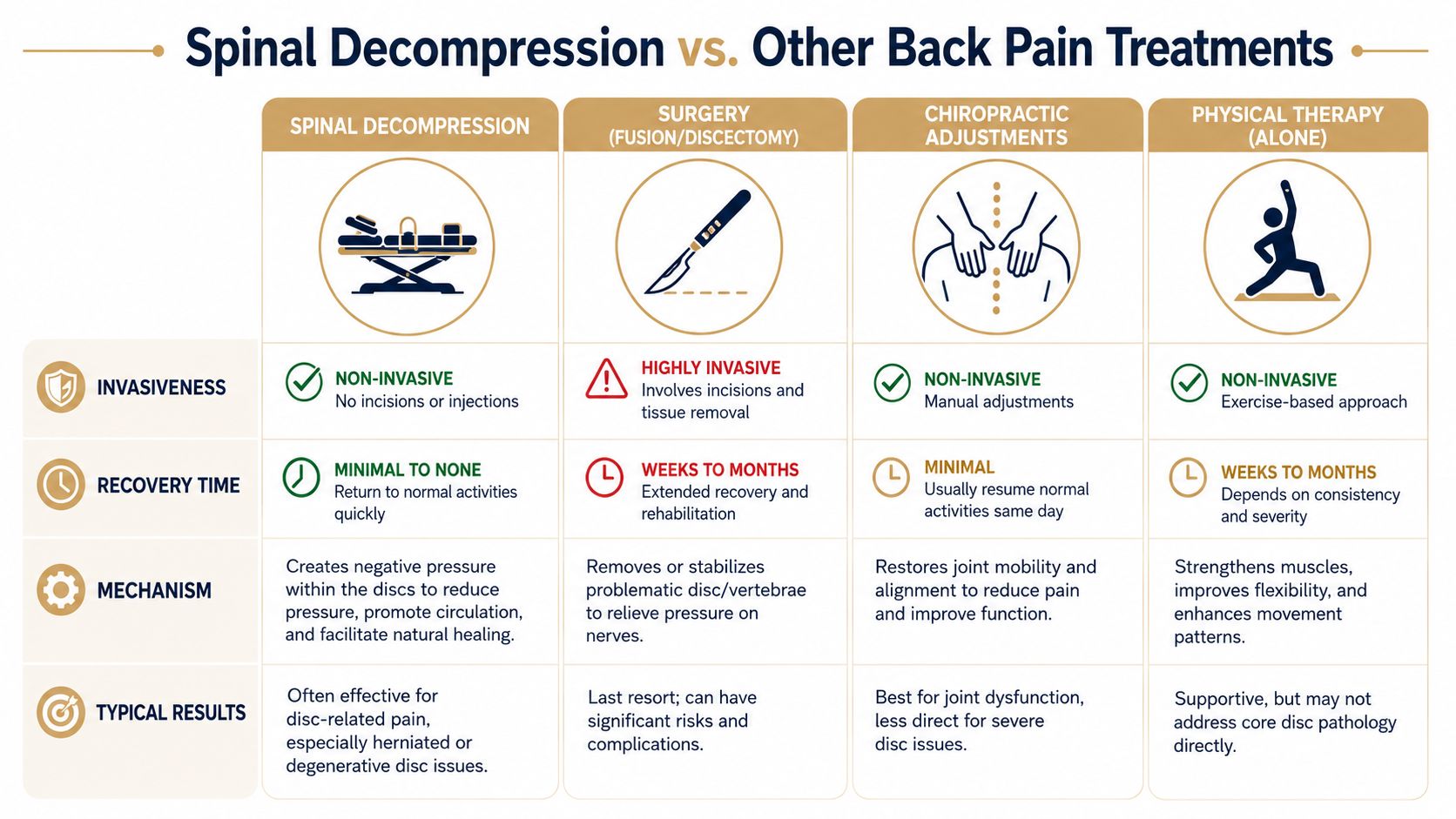
Surgery has an important role. When someone has major neurological compromise, severe structural compression, or a condition that doesn't belong in conservative care, surgery may be necessary. But surgery is invasive and usually reserved for situations where risk, anatomy, and symptom severity justify it.
Decompression sits in a different category. It's non-surgical, structured, and intended to reduce disc-related pressure without removing tissue or stabilizing the spine surgically. For many patients, that makes it a reasonable step before discussing procedures.
A chiropractic adjustment and decompression do different jobs. An adjustment is often useful when joint restriction, guarded movement, or segmental dysfunction is part of the pain pattern. It can improve motion and reduce mechanical irritation in the short term.
Decompression is more specific to cases where disc pressure appears central to the problem. If someone has radiating leg pain from a disc lesion, a skilled clinician may use both approaches, but not as interchangeable treatments.
Exercise is essential. It improves endurance, control, tolerance, and long-term resilience. It also addresses the problem many back pain patients live with after the acute flare settles, poor load management and poor spinal stability under real-life demands.
But exercise alone can be hard to tolerate in the wrong phase. A patient with irritable nerve pain may need symptoms quieted enough to move well first.
Here's the important nuance. There is limited scientific literature directly comparing motorized decompression to less expensive conservative options like structured exercise alone, and that gap supports using decompression as part of a broader plan that also includes manual therapy and rehabilitative exercise, as discussed in this review of non-surgical spinal decompression evidence.
| Option | Where it helps most | Main limitation |
|---|---|---|
| Spinal decompression | Disc-related compression patterns | Passive care alone doesn't build lasting stability |
| Surgery | Severe structural or neurological cases | Invasive, with recovery demands |
| Chiropractic adjustment | Joint restriction and movement dysfunction | Less direct for true disc pressure problems |
| Rehabilitation exercise | Long-term control and resilience | May be hard to start during high-irritability phases |
The mistake isn't choosing one category of care. The mistake is expecting one category to do every job.
For the right patient, decompression can open a window. Adjustments can restore motion where it's restricted. Massage therapy can reduce soft-tissue guarding. Muscle stimulation or MLS Laser Therapy may help calm symptoms enough for movement to improve. Rehabilitation exercise then gives the improvement somewhere to go.
That integrated model is more honest than saying a machine fixes spines by itself.
The biggest weakness in many decompression plans isn't the machine. It's the missing follow-through around it. A patient comes in for passive care, feels somewhat better, then goes back to the same movement habits, the same deconditioned support system, and the same pain triggers. That's how short-term gains disappear.
In a coordinated musculoskeletal clinic, decompression is one tool among several. A patient may also need:
That's also why managing your health care team matters. Patients do better when care isn't fragmented and each part of the plan supports the others.
The evidence gap isn't a reason to dismiss decompression. It's a reason to use it responsibly. If the literature doesn't prove that motorized decompression is superior to every conservative option by itself, then the logical response is not to oversell it. The logical response is to combine it with the approaches that support long-term function.
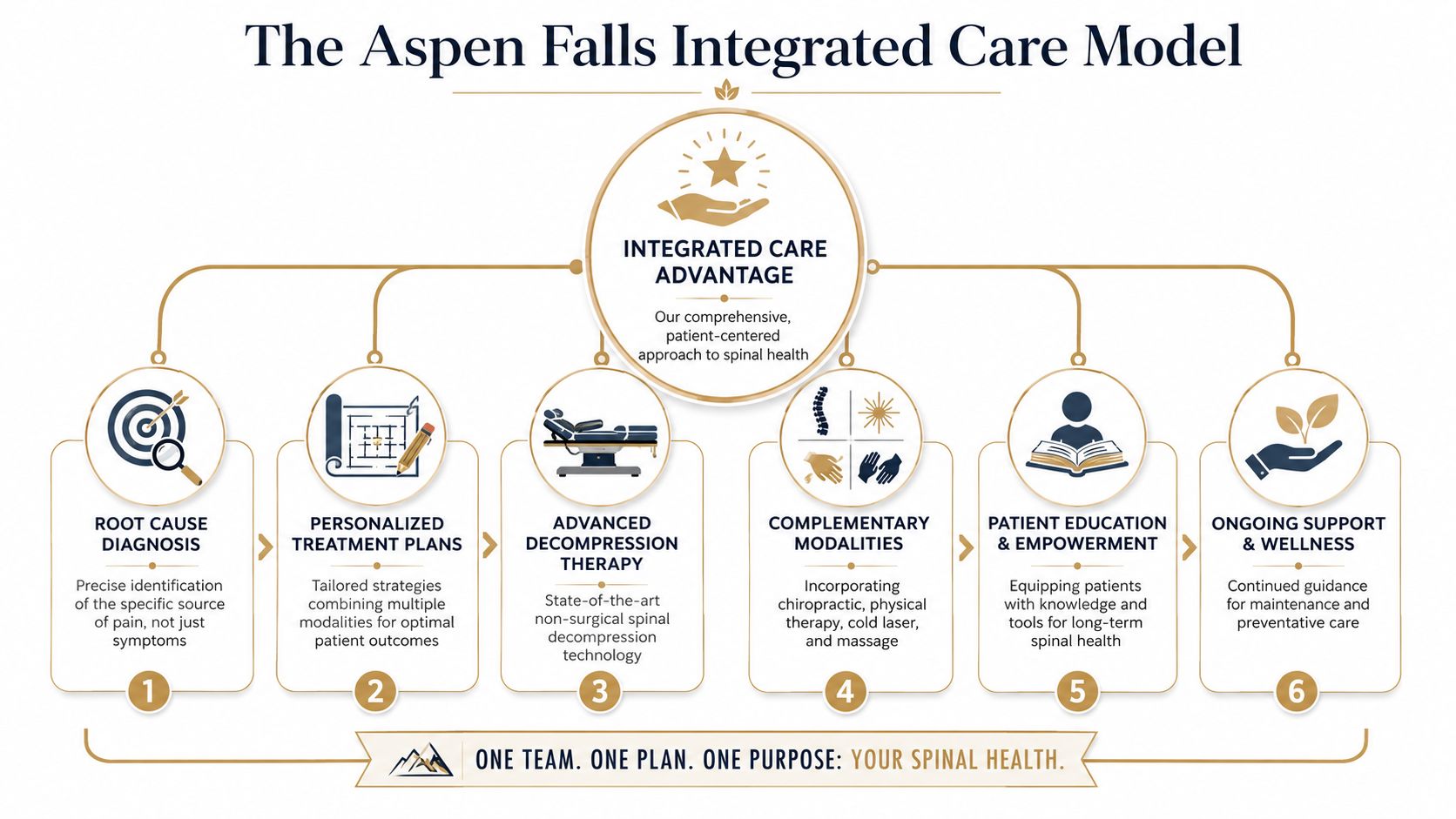
That's where a clinic such as Aspen Falls Wellness can fit for patients who want coordinated conservative care that combines spinal decompression with chiropractic adjustments, mobility work, and active rehab.
A durable result usually follows a sequence like this:
Passive care can lower the noise. Active care changes the pattern.
That's the core advantage of an integrated plan. It respects what decompression does well, and it doesn't ask decompression to do work that belongs to exercise, manual care, or behavior change.
Most patients describe spinal decompression therapy as a gentle, controlled pulling sensation. It shouldn't feel aggressive. Some people feel mild soreness after early visits, especially if they've been moving poorly for a while, but the treatment itself is generally meant to be tolerable.
Some patients notice change early. Others need a number of sessions before the pattern starts to shift. The better question is whether relief is becoming more consistent, whether leg symptoms are centralizing, and whether daily activities are getting easier. Those trends matter more than a dramatic first session.
This is the question many clinics avoid because the honest answer is nuanced. Many patient FAQs fail to address the core question of realistic surgery avoidance compared to structured exercise alone. The key point is that outcomes are more likely to improve when passive modalities like decompression are combined with active rehabilitation that addresses the underlying instability pattern, as discussed in this patient FAQ discussion on decompression and active rehab.
Coverage depends on your plan and the way services are billed. Some components of care may be covered while others may not be. The only useful answer is a real benefits check before starting. Ask for clarity on what's covered, what isn't, and whether home exercise, massage, chiropractic care, or other services are part of the financial picture.
Keep it simple:
Yes, and for many patients it should be. Depending on the exam, a plan may include chiropractic care, sciatica treatment, rehabilitation exercise, mobility therapy, massage therapy, acupuncture, nutrition support, or car accident treatment if the problem began after a collision.
If you're trying to decide whether spinal decompression therapy belongs in your treatment plan, the next step is a proper diagnosis and a realistic discussion of options. Aspen Falls Wellness provides non-surgical musculoskeletal care in Salt Lake City and Sandy, including DRX 9000 spinal decompression, chiropractic adjustment, massage therapy, MLS Laser Therapy, SoftWave Therapy, rehabilitation exercise, mobility therapy, acupuncture, nutrition counseling, and related pain relief services within a coordinated care model.

Stay updated with the latest chiropractic news and exclusive offers.





