
After a car crash? Get a clear plan for car accident injury treatment. Explore non-surgical options, including chiropractic, DRX9000, and claims help.
You walk away from the crash feeling shaky but relieved. The ER ruled out anything life-threatening. Maybe the X-rays were “normal,” you were told to rest, and now you're home wondering why your neck is tightening, your lower back is starting to ache, or turning your head feels strangely guarded.
That experience is common. The first part of a collision is chaos. The harder part often comes after, when the adrenaline wears off and the complete injury picture starts to surface. Consequently, many people err, assuming that if nothing was broken, they should just wait it out.
In practice, that's often the wrong move. Car accident injury treatment is not only about emergency care. It's about catching the soft-tissue, spinal, disc, and nerve-related problems that can turn into months of pain if they aren't identified early and treated correctly.
You get home after the crash, answer a few texts, and tell yourself you were lucky. The ER ruled out the immediate emergencies. The car can be dealt with tomorrow. Then the next morning you turn your head backing out of the driveway and realize your neck does not move normally. By that night, your low back tightens, your shoulders burn, or a headache settles in behind your eyes.
I hear this sequence often in practice. The first hours after a collision are crowded with police reports, insurance calls, photos, towing, and family updates. In that rush, many injured people judge their condition by one question. “Can I still function?” Right after a crash, that is not a reliable test.
Adrenaline changes what you feel. So does muscle guarding. In the early stage, the body is trying to protect injured areas, not give you a clear mechanical report. Symptoms often surface later, once the nervous system settles down and inflamed tissue starts reacting to the force it absorbed.
A common early pattern looks like this:
Delayed pain still counts as accident pain.
That matters because the period after the ER is where many long-term problems begin. If life-threatening injuries have been ruled out, the next job is to identify what the crash did to your joints, muscles, discs, and supporting soft tissue before stiffness turns into a chronic pattern. “No broken bones” is good news. It is not the end of the evaluation.
The practical next step is simple. Pay attention to new pain, reduced motion, headaches, numbness, sleep changes, and pain that worsens over 24 to 72 hours. Those signs deserve follow-up, even if you walked away from the scene. Early treatment is often the difference between a short recovery and months of lingering neck or back pain.
Emergency care saves lives. It is not the same thing as a full musculoskeletal evaluation.
Many patients hear “no fracture” and assume that means “no real injury.” That assumption creates one of the biggest problems in post-collision care. The body can sustain substantial soft-tissue and spinal injury even when standard imaging doesn't show a broken bone.

An emergency department is built to answer urgent questions fast. Is there a fracture? Internal bleeding? A brain injury that needs immediate intervention? A major neurological emergency?
That focus is appropriate. But it leaves a diagnostic gap once life-threatening issues have been ruled out. As described in this discussion of post-crash soft-tissue care, standard X-rays often fail to detect micro-tears and vertebral subluxations, and many people are discharged believing they're uninjured when the underlying problem is hidden in the soft tissue and spinal mechanics.
A useful analogy is a house after an earthquake. The foundation may still be standing, but there can be cracks behind the drywall, strain through the frame, and doors that no longer close properly. Your spine and soft tissues can respond the same way after a collision.
These are some of the problems that often live in that gap:
| Injury pattern | What you may feel | Why it matters |
|---|---|---|
| Whiplash-related ligament strain | Neck stiffness, headache, pain turning the head | Untreated instability and guarding can drive chronic pain |
| Disc irritation or herniation | Low back pain, sciatica, pain with sitting | Pressure on irritated nerves can worsen functional loss |
| Muscle and fascial injury | Tightness, spasm, pulling pain, restricted motion | Scar tissue can form in a disorganized way if movement isn't restored |
| Joint misalignment or subluxation | Localized pain, reduced range of motion, uneven movement | Poor mechanics keep surrounding muscles overworking |
When people “wait and see,” the body doesn't always sort this out cleanly. Injured tissue stiffens. Muscles compensate. You start moving around the pain instead of through a proper recovery. That's how an acute injury becomes a chronic pattern.
Practical rule: If the ER ruled out danger but your movement, sleep, or daily function is getting worse, you need a second-stage evaluation, not more waiting.
A proper post-crash evaluation feels very different from an ER visit. It should be slower, more detailed, and focused on function.
The first step is a detailed history. Not just where it hurts, but how the crash happened, where you were struck, whether you were braced, what symptoms started right away, and what changed over the next several days. That mechanism matters because rear-end, side-impact, and rotational collisions load the body differently.
Then comes the physical exam. A thorough visit usually includes:
If spinal alignment or postural mechanics are part of the problem, a patient-friendly comprehensive guide to spinal alignment can help you understand why even subtle positional changes can create larger pain patterns over time.
The point of this evaluation isn't just to attach a diagnosis label. It's to build a treatment plan that matches what your body is doing.
Sometimes that means digital X-rays to study spinal positioning more carefully. Sometimes it means an MRI referral when disc injury, radicular pain, or persistent neurological symptoms suggest deeper soft-tissue involvement. Sometimes it means your exam points strongly toward whiplash mechanics, in which case targeted care matters more than more rest. If that's your pattern, this overview of whiplash injury treatment can help you understand what early conservative care usually involves.
A thorough evaluation should also tell you what isn't indicated. Not every patient needs decompression. Not every sore neck needs aggressive manipulation on day one. Not every low back flare is a surgical case. Good care starts by narrowing the problem correctly.
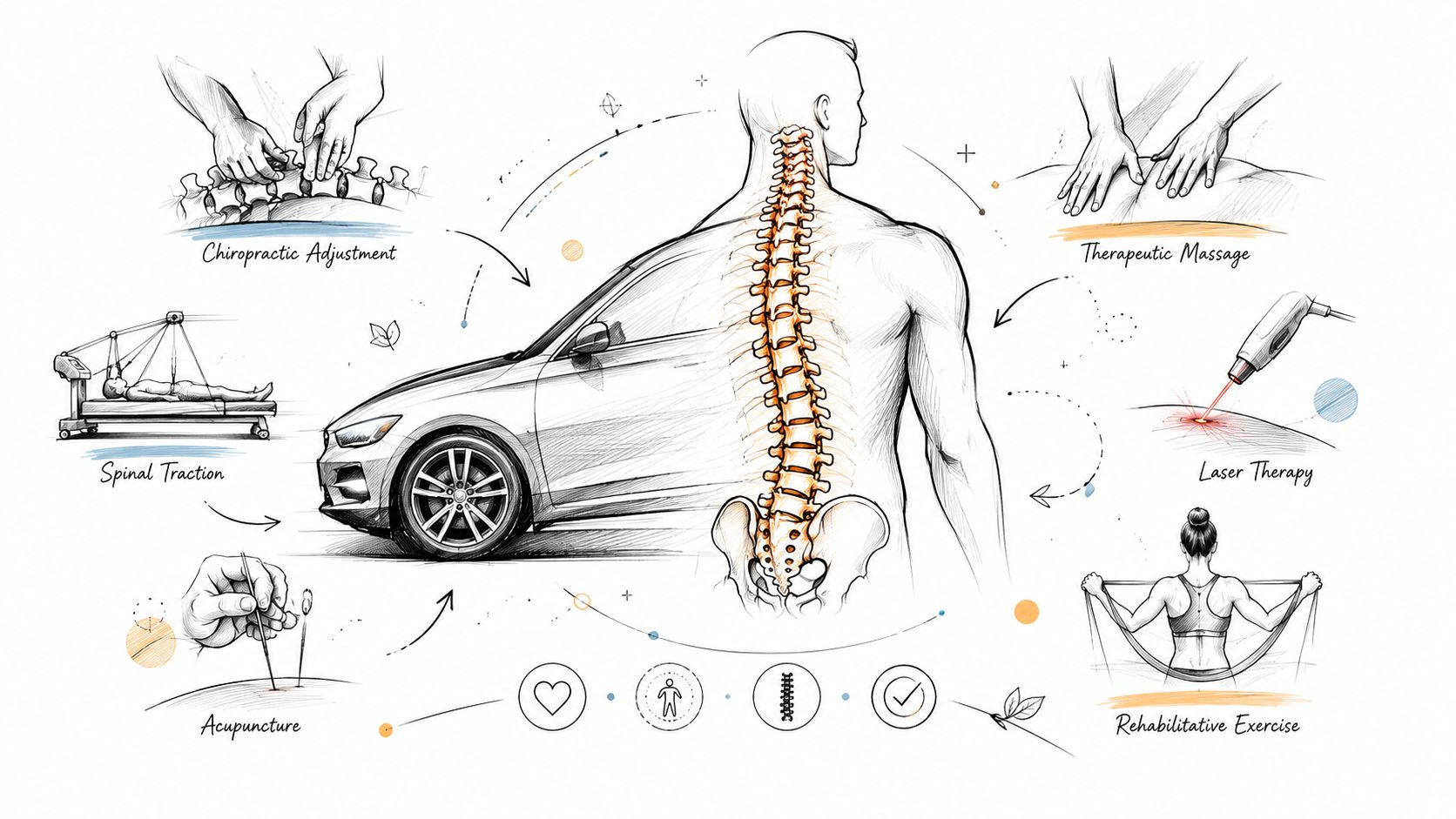
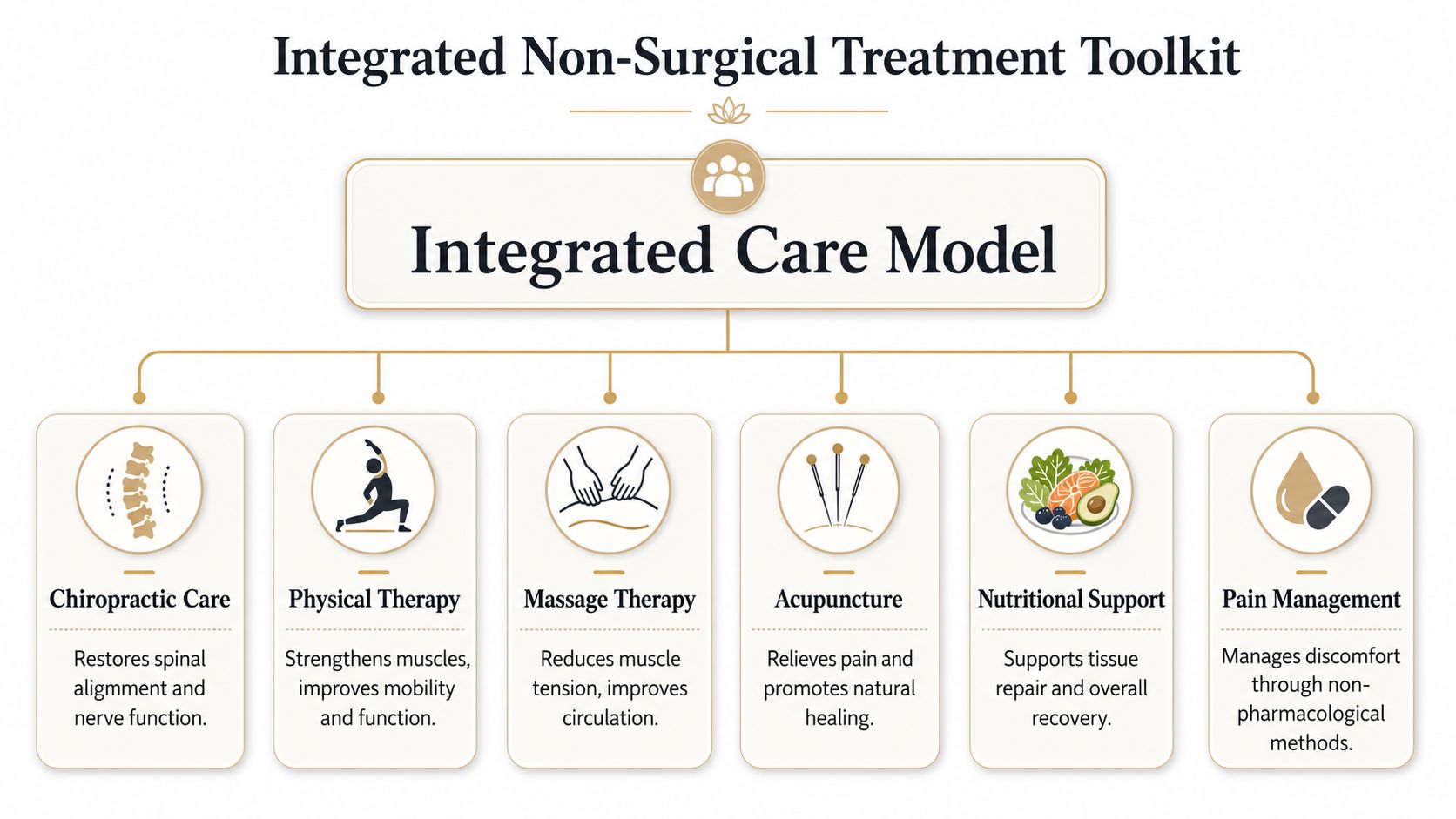
Once the injury pattern is clear, treatment works best when it is integrated rather than pieced together. A car crash rarely injures only one tissue. The spine, muscles, fascia, joints, and nerves all react together. That's why the most effective non-surgical care plans combine several tools instead of relying on one.
Chiropractic care has an important role after an accident when it is applied thoughtfully and matched to the stage of healing. A chiropractic adjustment can help improve joint motion in areas that became restricted after impact. Realignment work is useful when the spine is moving asymmetrically and surrounding muscles are overcompensating.
Hands-on treatment is often broader than an adjustment alone. It may include:
The trade-off is important. Passive treatment can lower pain, but passive treatment alone rarely rebuilds durable function. It creates an opening. The next step is using that opening well.
Some post-accident cases need more than manual care. This is especially true when the crash has aggravated a lumbar disc, created sciatica, or produced persistent nerve compression symptoms.
For the right patient, Spinal Decompression with the DRX 9000 is one of the most useful non-surgical options. In car accident-related lumbar disc herniation or sciatica, non-surgical spinal decompression using the DRX9000 generates intradiscal pressures of −150 to −200 mmHg, creating a pressure gradient that can help retract herniated disc material and reduce nerve root compression. Clinical cohorts reported 70 to 80 percent success in pain reduction and functional improvement within 6 to 12 weeks, as summarized in this DRX9000 and trauma care reference.
That doesn't make decompression a universal answer. It is most appropriate when the exam supports disc involvement, the patient is a good candidate, and the goal is to relieve pressure without moving toward surgery too quickly. If you want a closer look at how that process works, this page on spinal decompression therapy explains the treatment approach in more detail.
Other tools can support healing in different ways:
At Aspen Falls Wellness, this kind of care is typically organized as a coordinated plan rather than isolated visits. That matters because a disc problem, a whiplash pattern, and a guarded thoracic spine each respond to different combinations of treatment.
The right therapy is the one that matches the tissue involved, the stage of healing, and the patient's tolerance that day.
The final piece is the part many patients underestimate. Rehabilitation exercise is what turns symptom relief into actual recovery.
A strong plan usually includes:
For active patients, even specialty services such as golf movement screening can matter later in recovery. Not because golf is urgent after a crash, but because your return to full movement has to include the things you want your body to do.
The question almost every injured patient asks is simple. How long is this going to take?
The honest answer is that recovery is individual. The more useful answer is that patients typically improve in phases, and each phase has a different job. When patients understand that sequence, they stop judging recovery only by day-to-day pain fluctuations.

The first phase is about reducing inflammation, controlling pain, and protecting irritated structures without slipping into complete inactivity. During this stage, gentle treatment, careful movement, and the right diagnosis are paramount.
For post-collision whiplash, timing matters. Early initiation of active rehabilitation within 7 to 10 days significantly reduces the risk of chronic neck pain compared with prolonged immobilization, and patients receiving combined manual therapy with graded exercise achieved 30 to 40 percent greater improvement in Neck Disability Index scores at 6 weeks, according to this motor vehicle accident injury treatment review.
That finding matches what we see clinically. Too much rest often backfires. The neck gets stiffer, the patient gets more fearful of movement, and recovery slows.
Early movement should be guided, not aggressive. There's a big difference between doing too much and doing nothing.
Once pain is less reactive, treatment shifts. The goal becomes restoring normal mechanics, strength, and confidence in movement.
A typical progression may look like this:
| Recovery phase | Main focus | Common tools |
|---|---|---|
| Acute phase | Calm pain, reduce irritation, stabilize | Gentle adjustment, massage therapy, laser therapy, soft tissue care |
| Sub-acute phase | Restore motion and tolerance | Mobility therapy, rehabilitation exercise, chiropractic care |
| Restorative phase | Build strength and endurance | Personal exercise plans, muscle stimulation, progressive activity |
| Maintenance phase | Prevent recurrence | Home exercise, posture work, nutrition counseling, periodic re-evaluation |
The timeline changes based on the injury. A straightforward strain behaves differently than a disc injury with sciatica. A headache-driven whiplash pattern behaves differently than a shoulder and thoracic restriction problem. What matters most is that the plan gets updated as your body changes.
If inflammation has been a major barrier, some patients also benefit from learning when therapies such as laser therapy for inflammation fit into the broader rehab process. The point is not to collect treatments. The point is to use each one at the right stage.
After the ER visit, many patients hear some version of, "Nothing is broken," then assume the paperwork can wait. That is a mistake I see often. Soft tissue injuries, joint irritation, headaches, nerve symptoms, and delayed stiffness may not look dramatic on day one, but they still need a clear medical record if you want your treatment and your claim to reflect what your body is experiencing.
Insurance decisions are built on documentation. Pain alone is not enough. Your records need to show when symptoms started, how they changed, what findings were present on examination, what treatment was recommended, and how the injury affected daily life.
Start a file early and keep it organized. The goal is simple. Make it easy to show a consistent timeline from the crash to your recovery.
If you are still organizing report details or confirming background information tied to the collision, VekTracer's instant history checks can be a useful reference while you sort your records.
A claim gets stronger when the medical timeline makes sense. Prompt evaluation, a detailed initial examination, follow-up visits, and periodic re-checks all help show that the injury was real, persistent, and medically significant.
Gaps create problems.
From a clinical standpoint, delayed care can let stiffness, guarding, and altered movement patterns settle in. From an insurance standpoint, long breaks in treatment give the carrier room to argue that the problem resolved, came from something else, or was never serious enough to require care.
I tell patients to be accurate, not dramatic. If your neck pain is improving but you still cannot turn your head comfortably while driving, say that. If your low back pain is intermittent but flares every time you sit for more than 20 minutes, document that pattern. Specific details carry more weight than broad statements like "still sore."
The strongest file is usually the clearest one. Early records. Specific symptoms. Consistent follow-up. Measurable functional limits. If your recovery takes time, your documentation should show why.
A crash can leave you dealing with two problems at once. One is pain. The other is uncertainty. You may not know whether your symptoms are “serious enough,” whether you need imaging, whether conservative care is enough, or whether you're doing too little or too much.
That uncertainty is exactly why local follow-up matters. In the European Union, injuries leave approximately 1 million people permanently disabled each year, according to the EU injury data report. The lesson for patients is straightforward. Early, effective rehabilitation is not optional if you want to lower the chance of long-term limitation.
If you're choosing a provider for car accident injury treatment in Salt Lake City, look for a clinic that can do more than a quick adjustment and a handout.
You want care that includes:
If legal questions are part of your situation, Ares' insights on back injury cases can help you understand how injury severity and documentation often shape the broader claim process.
Make the appointment if your pain is worsening, your movement is shrinking, your sleep is disrupted, or you're noticing headaches, numbness, sciatica, or persistent stiffness after the crash. Make it if the ER said you were fine but your body says otherwise. Make it if you're trying to avoid medication escalation or surgery and want to know what conservative care can realistically do.
The goal isn't to over-treat. It's to identify the specific injury, use the least invasive tools that fit the problem, and help you get back to normal life without carrying crash pain longer than you should.
If you're dealing with lingering pain, stiffness, headaches, sciatica, or reduced mobility after a collision, schedule a detailed evaluation with Aspen Falls Wellness. The clinic provides non-surgical musculoskeletal care in Salt Lake City and Sandy, with treatment options that can include chiropractic care, DRX 9000 spinal decompression, MLS Laser Therapy, SoftWave Therapy, massage therapy, acupuncture, mobility therapy, nutrition counseling, and personalized rehabilitation plans.

Stay updated with the latest chiropractic news and exclusive offers.





