
Explore disc herniation treatment options for 2026. Find conservative care, chiropractic, spinal decompression, or surgery. Learn risks, benefits & choose your
You may be reading this with a fresh MRI result in your hand, or after a week of back pain that suddenly started shooting into your hip, leg, or foot. Maybe someone told you that you have a “herniated disc,” and now you're wondering whether you need surgery, an injection, rest, chiropractic care, or something more advanced.
That uncertainty is normal. The good news is that a disc problem doesn't typically necessitate immediate invasive care. The better news is that disc herniation treatment options make a lot more sense when you organize them by timing, severity, and response, instead of treating them like a random menu of therapies.
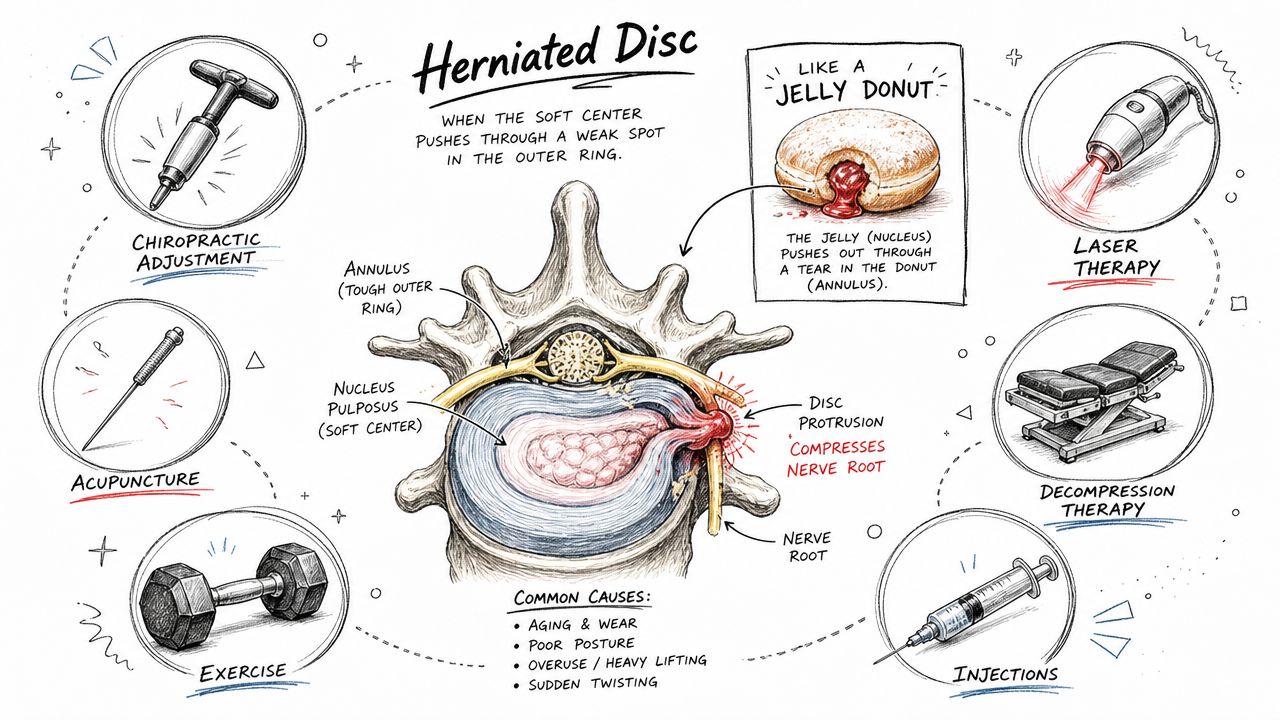
A disc herniation sounds dramatic because the name is dramatic. In plain language, it means part of the soft inner material of a spinal disc has pushed outward through a weaker area of the disc wall and is now irritating or compressing a nearby nerve.
The easiest way to picture it is a jelly donut. The outside is the tougher ring. The inside is softer. If pressure builds and the outer layer weakens, some of that inner material pushes outward. In your spine, that can trigger local pain, muscle spasm, numbness, tingling, or radiating pain like sciatica.
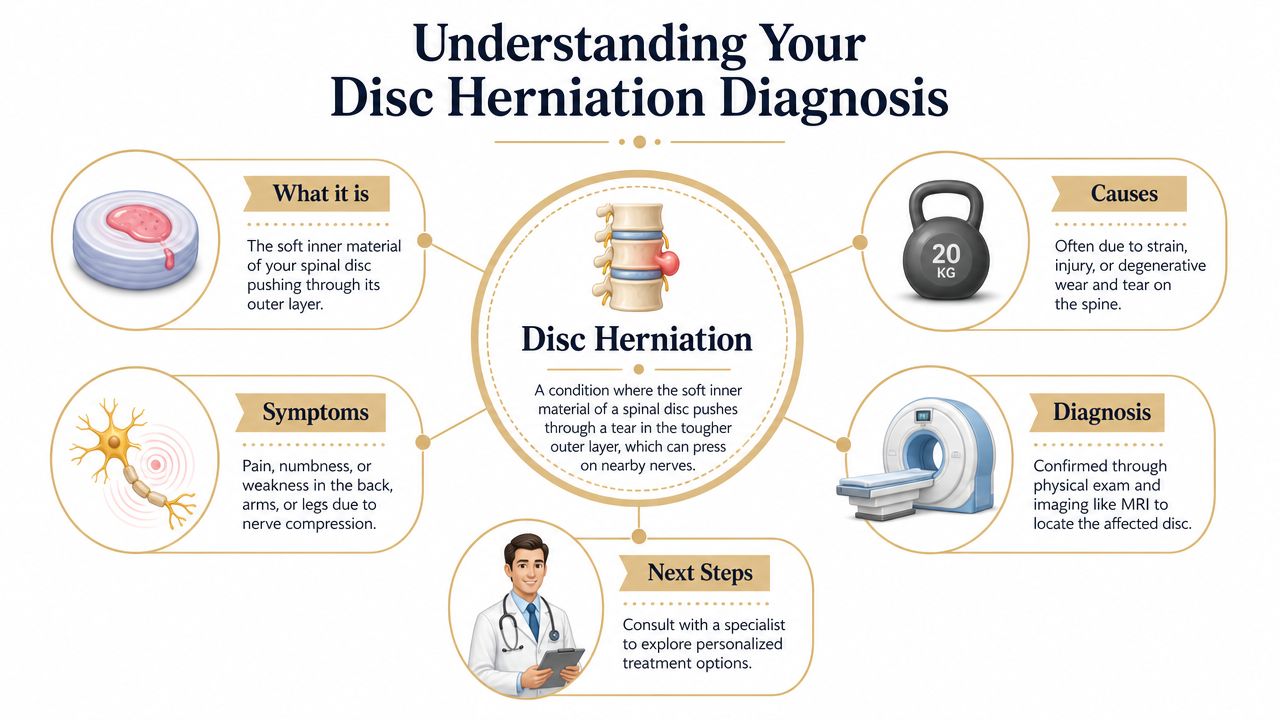
Back pain from a disc isn't always just “back pain.” If the disc presses on a nerve root, pain can travel down the leg or arm. That's why one person feels aching across the low back, while another feels burning into the calf or numbness in the foot.
That also explains why treatment has to focus on more than the spot that hurts. If the nerve is irritated, the goal is to reduce pressure, calm inflammation, restore motion, and help the body recover without provoking the area further.
Practical rule: Severe symptoms don't automatically mean severe treatment. The first question is whether the nerve is irritated, failing, or in danger.
A diagnosis should also lower your fear, not raise it. Approximately 90% of patients newly diagnosed with lumbar disc herniation experience initial symptom relief through conservative treatment according to this clinical review on lumbar disc herniation management.
Once a disc herniation is identified, the real task is deciding where you fit on the care pathway. Some patients improve with activity changes, anti-inflammatory support, hands-on care, and guided exercise. Others need decompression, injections, or a surgical consult because symptoms keep progressing.
If getting to the office is difficult, secure virtual follow-up can help you stay on track between visits. Resources like AONMeetings' HIPAA telehealth solutions are useful for understanding what safe remote care coordination should look like.
If your main symptom is radiating leg pain, this guide on whether a chiropractor can help sciatic nerve pain can help you connect the diagnosis to what you're feeling day to day.
In the absence of major neurological loss or emergency warning signs, conservative care is the right starting point. That isn't a “wait and hope” strategy. It's an active plan built around symptom control, movement restoration, and protecting the irritated disc while it settles.
Evidence supports that approach. In patients with lumbar disc herniation who don't have neurological deficits or cauda equina syndrome, conservative management is the first-line treatment, and approximately 60 to 90% of cases resolve spontaneously within 6 weeks as the herniated material undergoes resorption, based on this WFNS-aligned review of lumbar disc herniation care.
The first phase has a simple purpose. Calm the nerve down enough that you can move better, sleep better, and start rebuilding function.
That usually means combining several tools rather than relying on one:
Patients often get stuck because they pick the wrong kind of rest. Short-term unloading can help. Prolonged inactivity usually doesn't.
A few common mistakes slow recovery:
Recovery usually improves when patients stay active within tolerance, change positions often, and follow a plan that matches their symptom pattern instead of forcing movement.
A practical conservative program usually includes a mix of in-office care and home care. The exact combination varies, but the pattern is consistent.
| Focus | Why it matters |
|---|---|
| Pain relief | Reduces guarding so you can move more normally |
| Motion restoration | Prevents the surrounding joints from stiffening up |
| Disc unloading | Lowers pressure on the irritated nerve |
| Core and hip control | Reduces repeat stress on the spine |
| Activity modification | Keeps you healing without shutting life down |
At this stage, services like sciatica treatment, decompression, chiropractic care, massage therapy, acupuncture, mobility therapy, and rehabilitation exercise all have a role when they're selected for a clear reason, not used as a one-size-fits-all package.
Some patients do all the right first-line things and still hit a wall. They're not in crisis, but they're also not recovering well enough. That's where more targeted non-surgical options become useful.
The key question isn't whether a modality sounds high-tech. It's whether it addresses the specific problem that's still driving symptoms. In disc cases, that problem is often ongoing nerve irritation, disc pressure, inflammation, and poor tissue recovery.
Non-surgical spinal decompression is most relevant when the disc itself is still a major pain generator and standard manual care alone hasn't created enough change. The aim is controlled unloading of the affected spinal segment.
For patients researching disc herniation treatment options, DRX9000 spinal decompression gets attention because it is designed to create negative pressure within the disc space, which may help reduce stress on the involved tissue and improve conditions around the irritated nerve. In a cohort study of 30 patients with discogenic low back pain, DRX9000 reduced average pain scores from 6.2 to 1.6, with a treatment success rate exceeding 75%, according to this study summary on DRX9000 outcomes.
That doesn't mean every patient with a herniated disc needs decompression. It means decompression can be a reasonable next step when pain persists, sitting is difficult, leg symptoms remain active, or repeated flare-ups suggest the disc still isn't tolerating normal load well.
If you want a closer look at how this approach is used in practice, this page on spinal decompression therapy outlines the basic treatment concept.
Decompression addresses load. Other modalities are aimed more at the tissue response.
MLS Laser Therapy is commonly used to reduce inflammation and support recovery in deeper tissues. In practice, it can be helpful when the disc problem has triggered a larger pain pattern involving muscles, fascia, and irritated nerve pathways.
SoftWave Therapy serves a different role. It's used to stimulate tissue repair and healing support at a cellular level. That makes it worth considering when a patient is no longer in the earliest acute phase but still has stubborn tissue sensitivity or slow recovery.
A useful advanced treatment should answer a specific clinical question. Is the problem still pressure, still inflammation, still poor tissue healing, or a combination of all three?
Advanced modalities work better when they aren't isolated from the rest of care. They should support movement, not replace it.
A sound plan often combines:
Aspen Falls Wellness is one example of a clinic model that combines DRX9000 spinal decompression, SoftWave Therapy, MLS Laser Therapy, chiropractic adjustment, and home exercise within one non-surgical pathway.
Injections occupy an important middle ground. They are more invasive than office-based conservative care, but less invasive than surgery. Used well, they can reduce enough pain to let a patient re-engage with rehab.
Used poorly, they become a cycle of short-term symptom suppression with no meaningful change in the underlying mechanics.
For patients who don't improve enough with an initial trial of conservative care, epidural steroid injections are considered a viable second-line option after 3 to 4 weeks of conservative management, with translaminar epidural injections and selective nerve root blocks indicated for symptoms lasting 4 to 6 weeks, as summarized in the evidence review cited earlier.
That timing matters. An injection isn't usually the first move for a new disc herniation. It becomes more relevant when nerve pain remains intense enough that walking, sleeping, or participating in treatment is difficult.
An epidural steroid injection doesn't remove the disc herniation. It aims to reduce inflammation around the affected nerve root.
That can help in several ways:
The best use of an injection is as a bridge. It creates a window where you can move, strengthen, and recover more effectively.
If an injection helps but nothing else changes, symptoms may return once the temporary benefit wears off. That's why interventional pain management should usually sit inside a broader plan that includes activity modification, mobility work, decompression when appropriate, and progressive exercise.
For the right patient, that bridge can be valuable. It just shouldn't be mistaken for the whole road.
Surgery has a real and appropriate role in disc care. The mistake is going to surgery too fast, or refusing to consider it when the nerve is clearly failing. Good decision-making is more useful than blanket opinions.
The strongest surgical conversations happen when the reason is clear. Progressive weakness, major neurological compromise, cauda equina syndrome, or persistent disabling symptoms despite appropriate non-surgical care all change the picture.
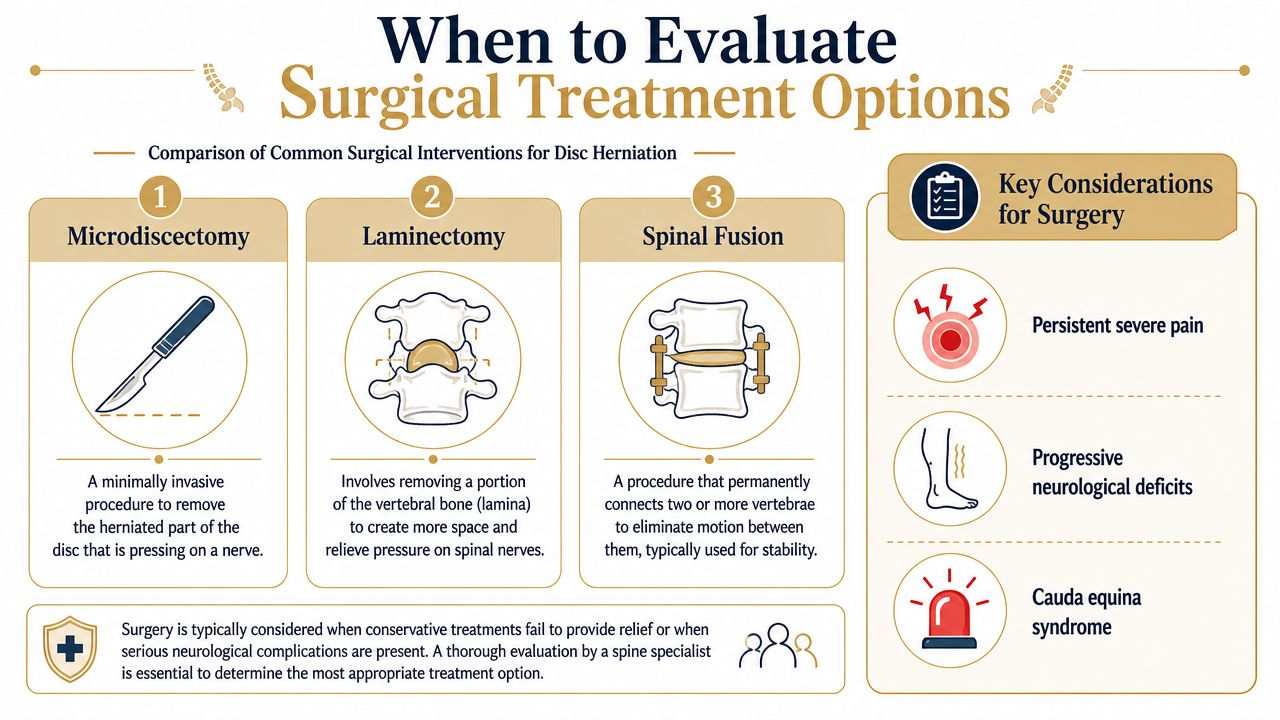
The most common operation for a disc herniation is some form of discectomy. The surgeon removes the portion of disc that is pressing on the nerve. In many cases, that means microendoscopic discectomy, which has a strong track record.
A review of surgical and non-surgical outcomes for lumbar disc herniation reports that microendoscopic discectomy has an approximate success rate of 90% and offers superior pain relief compared to conservative treatment within the first 6 months of symptoms, though long-term results beyond one year appear similar.
Other procedures may be considered depending on the anatomy and the reason for surgery:
| Procedure | Main goal | Best fit |
|---|---|---|
| Microdiscectomy or microendoscopic discectomy | Remove disc material compressing a nerve | Leg-dominant nerve pain from a focal disc herniation |
| Laminectomy | Create more room around the nerve structures | Cases where bony narrowing contributes to compression |
| Spinal fusion | Stabilize a painful or unstable segment | Cases involving instability, recurrent issues, or structural problems beyond a simple disc fragment |
Microdiscectomy is usually favored when the problem is a single herniated disc compressing a nerve because it directly addresses the compression without creating the longer recovery that fusion can require.
The trade-off is this. Surgery often gives faster symptom relief, especially in the earlier months. Long-term, the gap between surgical and conservative outcomes narrows for many patients. So the decision often comes down to urgency, severity, neurological findings, and how much disability remains after a good non-surgical trial.
There are situations where waiting is the wrong move:
Surgery isn't failure. It's one treatment option, and for the right patient, it can be the most efficient way to protect nerve function and restore quality of life.
Patients don't need more information. They need a decision framework.
The question isn't “Which treatment is best?” The question is “Which treatment fits my current stage, my symptoms, and my response so far?” Guidelines support surgery when conservative treatment fails or neurological impairment occurs, as outlined in this AAFP guidance on lumbar disc management.
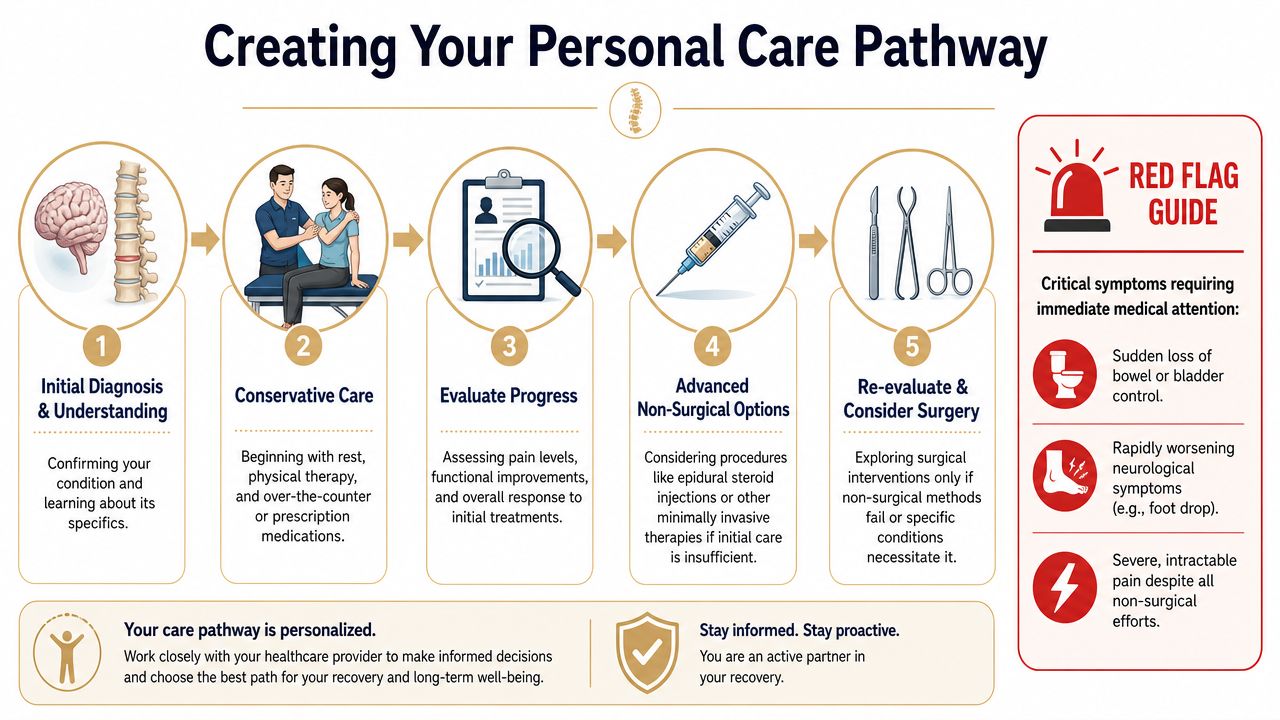
Some symptoms mean you shouldn't keep experimenting on your own.
Use this as a simple mental checklist:
There isn't one perfect deadline for every patient. Symptom severity, neurological findings, work demands, and response to treatment all matter.
A useful rule is to stay with conservative care when function is gradually improving and the nerve isn't failing. Consider moving up the ladder when pain remains intense, progress plateaus, or weakness appears.
Don't judge treatment by whether you had one good day or one bad day. Judge it by the weekly direction of pain, function, and nerve symptoms.
The most effective approach to disc care is usually conservative first, progressive when needed, and surgical only when the clinical picture justifies it. That keeps treatment proportional to the problem.
For local patients, the practical advantage is having access to a care model that can move from examination and diagnosis to chiropractic adjustment, decompression, massage therapy, acupuncture, mobility therapy, rehabilitation exercise, nutrition counseling, and car accident treatment when relevant, without losing the thread of the plan. If you're looking for local access, the Salt Lake City location page is the easiest place to start.
Disc herniation treatment options don't have to feel overwhelming when they're organized around one question: what is the next least invasive step that still makes clinical sense for your symptoms?
If you want help sorting out what stage you're in and which option fits, schedule a thorough evaluation with Aspen Falls Wellness. A clear diagnosis and a structured care pathway can make the difference between guessing and recovering.

Stay updated with the latest chiropractic news and exclusive offers.





